SCIENCE
Walk more, train more intensively, exercise together
Was die neue ESO-Leitlinie zur motorischen Rehabilitation nach Schlaganfall für Mobilität und Balance bedeutet

Jakob Tiebel
Health Business Consultant
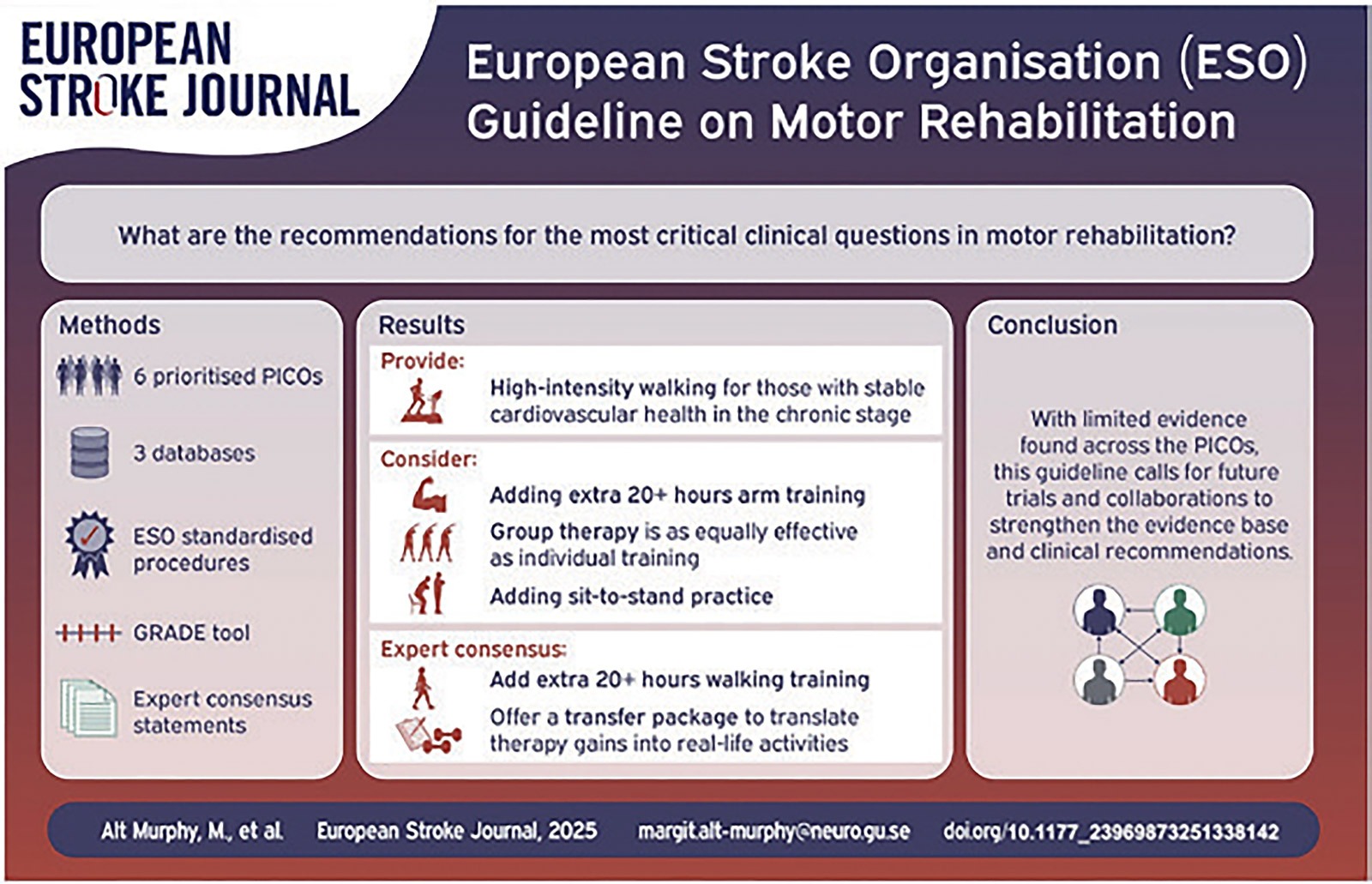
When people are asked what they most want back after a stroke, the answer is often not “more strength in my arm”, but to be able to walk safely again. Walking signifies independence, participation, dignity – and determines whether someone leaves their home or not. It is therefore all the more remarkable that until recently there was no independent European guideline explicitly dedicated to motor rehabilitation after stroke. This has changed with the European Stroke Organisation (ESO) guideline published in December 2025. The guideline on motor rehabilitation after stroke is the first of its kind and starts where everyday clinical practice has been calling for orientation for years: in terms of dosage, intensity, forms of organisation and motor functions relevant to everyday life. One message that is central to walking ability becomes particularly clear: More helps – but only if it is done properly.
At least 20 hours of additional gait training to improve walking ability.
Why this guideline is important
The new ESO guideline differs from many previous recommendations in that it does not attempt to cover “everything”. Instead, it concentrates on particularly relevant questions in clinical practice, known as PICO questions, including specifically walking, exercise intensity, group therapy and getting up from a sitting position. It was developed using standardised ESO procedures and the GRADE system, which transparently assesses the quality of the evidence. Where reliable studies are lacking, expert assessments are clearly labelled as such. This is an important step, especially for the rehabilitation of walking ability and balance: away from implicit assumptions and towards explicit, well-founded recommendations.
Anyone who wants to learn to walk again has to walk – at least 20 hours more
One of the key statements in the guideline concerns the dosage of gait training. Despite a heterogeneous study situation, the expert group came to a clear consensus: additional walking time improves walking ability after a stroke. Specifically, it is recommended that at least 20 additional hours of targeted gait training be planned in addition to the usual rehabilitation, typically spread over three to five sessions per week over four to six weeks.
This recommendation is noteworthy because it reveals an implicit deficiency in current practice: in many rehabilitation settings, there is simply not enough walking. Walking is often trained on a secondary basis, but not systematically, not repetitively and not to a sufficient extent. The guideline emphasises once again that walking ability is not a by-product, but must be trained in a targeted manner and for a sufficient period of time in order to achieve relevant improvements in walking distance, speed and endurance.
This recommendation is noteworthy because it reveals an implicit deficiency in current practice: in many rehabilitation settings, there is simply not enough walking. Walking is often trained on a secondary basis, but not systematically, not repetitively and not to a sufficient extent. The guideline emphasises once again that walking ability is not a by-product, but must be trained in a targeted manner and for a sufficient period of time in order to achieve relevant improvements in walking distance, speed and endurance.
Use transfer packages so that therapy successes become effective in everyday life.
Intensity counts – especially in the chronic phase
The guideline is even clearer when it comes to training intensity. For people in the chronic phase after a stroke who are cardiovascularly stable, it strongly recommends high-intensity gait training, at least with regard to walking endurance. There are also advantages for walking speed, albeit with a lower level of evidence.
What does “high-intensity” mean? It does not mean a leisurely walk in the corridor, but training at or close to one’s individual performance limit – for example on the treadmill, with speed targets or heart rate goals. The guideline sends a clear signal to practitioners: rest is not a therapeutic principle, at least not in the chronic phase. If the goal is to walk securely, the patient needs to be challenged.
This statement is particularly relevant because it contradicts the still widespread reluctance to engage in intensive exercise after a stroke. The ESO guideline makes it clear that with the right medical conditions, intensive gait training is not only safe but also effective.
What does “high-intensity” mean? It does not mean a leisurely walk in the corridor, but training at or close to one’s individual performance limit – for example on the treadmill, with speed targets or heart rate goals. The guideline sends a clear signal to practitioners: rest is not a therapeutic principle, at least not in the chronic phase. If the goal is to walk securely, the patient needs to be challenged.
This statement is particularly relevant because it contradicts the still widespread reluctance to engage in intensive exercise after a stroke. The ESO guideline makes it clear that with the right medical conditions, intensive gait training is not only safe but also effective.
Balance can be trained – through functional transitions and targeted exercise formats
In addition to walking, the guideline also focuses on postural balance as a key prerequisite for safe mobility. In particular, it emphasises the additional integration of sit-to-stand exercises. Repeatedly standing up and sitting down is highly relevant in functional terms, applicable to everyday life and can be used in various therapeutic contexts – from simple exercise settings to structured, device-based forms of training.
The guideline recommends including sit-to-stand training in addition to the usual therapy in order to specifically promote balance ability. Even if the duration, frequency and number of repetitions have not yet been clearly defined, the results emphasise that balance training is particularly effective when functional transitions are practised systematically, repetitively and progressively. This explicitly includes both manual and technically supported training approaches.
Sit-to-stand training can offer an easily manageable introduction to developing balance, strength and functional safety in parallel, especially for people with limited mobility. In practice, this principle can be flexibly extended – for example with device-based balance and standing training, which makes the number of repetitions, load and safety aspects precisely controllable, thereby enabling individualised progression.
The guideline recommends including sit-to-stand training in addition to the usual therapy in order to specifically promote balance ability. Even if the duration, frequency and number of repetitions have not yet been clearly defined, the results emphasise that balance training is particularly effective when functional transitions are practised systematically, repetitively and progressively. This explicitly includes both manual and technically supported training approaches.
Sit-to-stand training can offer an easily manageable introduction to developing balance, strength and functional safety in parallel, especially for people with limited mobility. In practice, this principle can be flexibly extended – for example with device-based balance and standing training, which makes the number of repetitions, load and safety aspects precisely controllable, thereby enabling individualised progression.
Training together – group therapy is not a compromise
Another practical aspect of the guideline concerns how therapy is organised. Contrary to the often implicit assumption that individual therapy is more effective per se, the available evidence shows that task-oriented group training for the lower limbs is at least as effective as individual therapy with a comparable duration – especially for balance, walking speed and walking endurance. The guideline makes a cautious but clear recommendation here. It is not the setting itself that is critical, but the quality of the training, the specific nature of the task and appropriate therapeutic supervision. This is an important message for clinical practice, as group therapy can not only be effective, but also resource-efficient and motivating for patients.
Supplement sit-to-stand training to specifically improve postural balance.
Transfer to everyday life – so that training remains effective
In addition to content-related and structural aspects of training, the guideline emphasises the importance of transfer packages. These are accompanying behaviour-oriented measures aimed at sustainably transferring therapeutic progress into everyday life. Even if the current evidence base is still limited, there is a broad consensus among experts that such transfer strategies can usefully support the effectiveness of motor rehabilitation.
A transfer package may include, for example, regular self-monitoring of activities, short reflection sessions, problem-oriented discussions, agreed exercise goals, home exercises that are relevant to everyday life and structured feedback loops. Especially when it comes to promoting mobility and balance, this approach can help to ensure that the skills developed during training are not limited to the therapy situation, but are actually used in the home and social environment.
In combination with task-oriented, repetitive and – where appropriate – technology-assisted training, this creates a framework that not only enables performance gains, but also systematically supports their implementation, stabilisation and further development in everyday life.
A transfer package may include, for example, regular self-monitoring of activities, short reflection sessions, problem-oriented discussions, agreed exercise goals, home exercises that are relevant to everyday life and structured feedback loops. Especially when it comes to promoting mobility and balance, this approach can help to ensure that the skills developed during training are not limited to the therapy situation, but are actually used in the home and social environment.
In combination with task-oriented, repetitive and – where appropriate – technology-assisted training, this creates a framework that not only enables performance gains, but also systematically supports their implementation, stabilisation and further development in everyday life.
What remains – and what should be changed
The ESO guideline does not conceal the fact that many recommendations are based on moderate to very low evidence. This is not a shortcoming of the guideline, but a reflection of the current state of research. At the same time, it formulates a clear mandate for research and practice: dosage, intensity and training organisation need to be investigated in a more targeted, comparable and internationally coordinated manner in future.
For clinical practice, however, the message is already clear:
If wanting to improve mobility and balance after a stroke, there is a need to walk more, train more intensively, practise functional transitions and question organisational barriers. The new ESO guideline does not provide simple recipes for this, but it does provide a clear compass.
Key recommendations for rehabilitation of the lower limbs
European Stroke Organisation (ESO) Guideline Motor Rehabilitation (2025)
1. Increase dosage and volume
In order to improve walking speed and walking endurance in the long term, the guideline recommends increasing the volume of gait training in a targeted manner. As a guide, at least 20 additional hours of specific gait training, spread over several weeks and supplementing the existing rehabilitation programme.
2. Use intensity in a targeted manner
High-intensity gait training is recommended for people in the chronic phase after a stroke who have a stable cardiovascular situation. This can significantly improve walking speed and, in particular, walking endurance, provided it is delivered safely, in a structured manner and with individualised adaptation.
3. Integrate sit-to-stand systematically
Additional repetitive sit-to-stand training is recommended to promote postural balance. Functional transitions such as standing up and sitting down play a central role in mobility, transfer safety and everyday skills, and can be implemented in different training settings.
4. Use targeted group therapy
Task-oriented group training for the lower limbs is at least as effective as individual therapy with a comparable duration, particularly with regard to walking speed, walking endurance and balance. Group settings can also positively support motivation, activity and therapy density – with appropriate supervision.
5. Promote activity beyond the therapy room
The guideline emphasises the importance of a high level of activity throughout the day. People who have had a stroke should be supported with being active for up to six hours a day through a combination of therapy, guided self-exercise and activities of daily living (ADL).
6. Train in an individual, goal-oriented manner
Rehabilitation should be consistently oriented towards the patient’s goals. Functional, repetitive and progressively designed training content that can be flexibly adapted to the level of performance, motivation and everyday requirements is crucial.
In order to improve walking speed and walking endurance in the long term, the guideline recommends increasing the volume of gait training in a targeted manner. As a guide, at least 20 additional hours of specific gait training, spread over several weeks and supplementing the existing rehabilitation programme.
2. Use intensity in a targeted manner
High-intensity gait training is recommended for people in the chronic phase after a stroke who have a stable cardiovascular situation. This can significantly improve walking speed and, in particular, walking endurance, provided it is delivered safely, in a structured manner and with individualised adaptation.
3. Integrate sit-to-stand systematically
Additional repetitive sit-to-stand training is recommended to promote postural balance. Functional transitions such as standing up and sitting down play a central role in mobility, transfer safety and everyday skills, and can be implemented in different training settings.
4. Use targeted group therapy
Task-oriented group training for the lower limbs is at least as effective as individual therapy with a comparable duration, particularly with regard to walking speed, walking endurance and balance. Group settings can also positively support motivation, activity and therapy density – with appropriate supervision.
5. Promote activity beyond the therapy room
The guideline emphasises the importance of a high level of activity throughout the day. People who have had a stroke should be supported with being active for up to six hours a day through a combination of therapy, guided self-exercise and activities of daily living (ADL).
6. Train in an individual, goal-oriented manner
Rehabilitation should be consistently oriented towards the patient’s goals. Functional, repetitive and progressively designed training content that can be flexibly adapted to the level of performance, motivation and everyday requirements is crucial.
Use high-intensity gait training to additionally improve walking ability.
Jakob Tiebel
Health Business Consultant
Jakob Tiebel is OT and studied applied psychology with a focus on health economics. He has clinical expertise from his previous therapeutic work in neurorehabilitation. He conducts research and publishes on the theory-practice transfer in neurorehabilitation and is the owner of an agency for digital health marketing.
References:
- Alt Murphy M, Munoz-Novoa M, Heremans C, Branscheidt M, Cabanas-Valdés R, Engelter ST, Kruuse C, Kwakkel G, Lakičević S, Lampropoulou S, Luft AR, Marque P, Moore SA, Podlasek A, Shankaranarayana AM, Shaw L, Solomon JM, Stinear C, Swinnen E, Turolla A, Verheyden G. European Stroke Organisation (ESO) guideline on motor rehabilitation. Eur Stroke J. 2025 Dec;10(4):1160-1188. doi: 10.1177/23969873251338142. Epub 2025 May 22. PMID: 40401760; PMCID: PMC12098312. l.ead.me/therapy-26-01-54 https://academic.oup.com/esj/article/10/4/1160/8377197
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.