
THERAPY-Magazin
Down with setup times!
A study on the THERA-Trainer lyra shows setup times average just 7 minutes, leaving more time for active therapy. Learn how small workflow changes significantly boost gait rehab efficiency for stroke patients.

Jakob Tiebel
Health Business Consultant
Therapy begins when the patient is actively training!
Background
Locomotion therapy is a key element of poststroke mobility rehabilitation. Intensive task-based gait training using an electromechanical gait trainer, such as the THERA-Trainer lyra, is at the forefront for patients unable to walk in the subacute phase. Electromechanical-assisted gait therapy has developed steadily over the past 20 years and is well documented.
Despite a largely similar structure and functional principle to the gait trainer systems available on the market, they are not directly comparable. For example, the technical complexity and the underlying operating concept determine the initial effort required for setup and transfer. Here, the use of modern gait robots is often both a curse and a blessing: against the backdrop of scarce resources and an average therapy time of around 30 minutes per gait therapy session, preparation and follow-up should be as fast as possible so that patients can practise as many steps as possible. That is, after all, the main objective. According to current recommendations, patients who are unable to walk should complete 800 to 1,000 steps per day. At least 20 minutes of active training time should be available for this purpose.
Locomotion therapy is a key element of poststroke mobility rehabilitation. Intensive task-based gait training using an electromechanical gait trainer, such as the THERA-Trainer lyra, is at the forefront for patients unable to walk in the subacute phase. Electromechanical-assisted gait therapy has developed steadily over the past 20 years and is well documented.
Despite a largely similar structure and functional principle to the gait trainer systems available on the market, they are not directly comparable. For example, the technical complexity and the underlying operating concept determine the initial effort required for setup and transfer. Here, the use of modern gait robots is often both a curse and a blessing: against the backdrop of scarce resources and an average therapy time of around 30 minutes per gait therapy session, preparation and follow-up should be as fast as possible so that patients can practise as many steps as possible. That is, after all, the main objective. According to current recommendations, patients who are unable to walk should complete 800 to 1,000 steps per day. At least 20 minutes of active training time should be available for this purpose.
Objective
The THERA-Trainer lyra comes with a very simple operating concept and short setup times, in line with its basic principle of being simple, effective and affordable. The aim of this task was to quantify this product promise as part of post-market clinical follow-up surveillance.
The THERA-Trainer lyra comes with a very simple operating concept and short setup times, in line with its basic principle of being simple, effective and affordable. The aim of this task was to quantify this product promise as part of post-market clinical follow-up surveillance.
Methodology and approach
In order to measure the mean setup times before and after a gait trainer session, the set-up times of a total of 33 sessions were recorded and evaluated in several neurological rehabilitation facilities in Germany in 2017.
The setup procedures were firstly standardised: 1) set up the safety belt; 2) place the patient in the lift system; 3) secure the feet in the foot plates; 4) lift the patient; 5) set body weight support; 6) set step length.
Depending on the patient’s degree of mobility, it was possible to set up the safety belt either for sitting or standing. This decision was made by the physiotherapist. Time recording always started at safety belt setup and ended at start of training.
After training, the patient was transferred from the gait trainer back to the wheelchair (the process described above in reverse). Here, time recording started when training stopped and ended when the patient was out of the safety belt.
In order to measure the mean setup times before and after a gait trainer session, the set-up times of a total of 33 sessions were recorded and evaluated in several neurological rehabilitation facilities in Germany in 2017.
The setup procedures were firstly standardised: 1) set up the safety belt; 2) place the patient in the lift system; 3) secure the feet in the foot plates; 4) lift the patient; 5) set body weight support; 6) set step length.
Depending on the patient’s degree of mobility, it was possible to set up the safety belt either for sitting or standing. This decision was made by the physiotherapist. Time recording always started at safety belt setup and ended at start of training.
After training, the patient was transferred from the gait trainer back to the wheelchair (the process described above in reverse). Here, time recording started when training stopped and ended when the patient was out of the safety belt.
In short – Functional Ambulation Categories (FAC) provide information about how much support a patient needs when walking
FAC 0 – The patient cannot walk or needs the assistance of two or more people. The walking distance – if walking is indeed realistic – is clearly and visibly less than 15 metres.
FAC 1 – The patient relies on continuous support of a person who helps to bear the weight and to maintain balance. An assistant provides support the whole time. This can be illustrated by a video recording, for example. Body contact is clearly visible at least once. The assistant clearly prevents the patient from falling. The assistant’s hand can be clearly seen supporting the leg or helping to bear the weight.
FAC 2 – The patient relies on continuous or intermittent assistance of a person for support with balance and coordination. No upper body contact or any support of body weight can be seen from the assistant. The assistant or physiotherapist places their hand or foot at least once on the patient’s leg. The assistant uses only hand contact to guard the patient.
FAC 3 - The patient relies on verbal support or assistance from one person, but direct physical help is not required. The assistant or physiotherapist does not make any hand or foot contact with the patient’s leg. No “hand contact” of any kind to guard the patient is allowed. But hands can be on standby.
FAC 4 - The patient walks independently on level surfaces with minimal help in the case of stairs or on difficult ground or surfaces, for example.
There is no identifiable contact or readiness by the assistant to intervene. It is possible for the patient to turn or rotate without assistance. On stairs and outdoors, however, walking is only possible with an assistant.
There is no identifiable contact or readiness by the assistant to intervene. It is possible for the patient to turn or rotate without assistance. On stairs and outdoors, however, walking is only possible with an assistant.
FAC 5 – The patient can walk independently in all contexts. This includes stairs and outdoor walking without an assistant.
Assessments
Functional Ambulation Categories (FAC) were used to determine the patient’s walking ability. The FACs are six different categories (0 to 5) that differentiate how much assistance a patient needs for walking, irrespective of the aids used. Category 0 refers to a patient who is completely unable to walk and category 5 refers to a patient who can independently handle all paths in the clinic, including stairs.
In addition to the FACs, the starting position (SP) was also documented for the subgroup analysis of the safety belt setup (subgroup: SP Sitting and SP Standing).
Functional Ambulation Categories (FAC) were used to determine the patient’s walking ability. The FACs are six different categories (0 to 5) that differentiate how much assistance a patient needs for walking, irrespective of the aids used. Category 0 refers to a patient who is completely unable to walk and category 5 refers to a patient who can independently handle all paths in the clinic, including stairs.
In addition to the FACs, the starting position (SP) was also documented for the subgroup analysis of the safety belt setup (subgroup: SP Sitting and SP Standing).
Patients
Patients were recruited on the basis of the severity of mobility impairment and independently of the etiology of the underlying disease.
The inclusion criteria required patients to have an underlying neurological disease and be aged 18 to 79 years. Patients had to be able to sit with their feet on the ground but not be able to walk independently: either not at all (FAC-0), with the help of two physiotherapists (FAC-1) or with the help of one physiotherapist (FAC-2). In addition, all patients had to have previously completed at least three training sessions.
The exclusion criteria were: acute confusion, acute medical need for treatment, subjective indication of circulatory overload in the assisted standing test, activated arthrosis of the large leg joints, severe spasticity of the large leg joints with an extension deficit for knee and hip > 30°, open areas in the area of padding or belt supports.
Every effort was made to include all eligible patients in the study period. The inclusion of at least 30 patients was planned – at least 10 patients in each subgroup of FAC 0-2.
Patients were recruited on the basis of the severity of mobility impairment and independently of the etiology of the underlying disease.
The inclusion criteria required patients to have an underlying neurological disease and be aged 18 to 79 years. Patients had to be able to sit with their feet on the ground but not be able to walk independently: either not at all (FAC-0), with the help of two physiotherapists (FAC-1) or with the help of one physiotherapist (FAC-2). In addition, all patients had to have previously completed at least three training sessions.
The exclusion criteria were: acute confusion, acute medical need for treatment, subjective indication of circulatory overload in the assisted standing test, activated arthrosis of the large leg joints, severe spasticity of the large leg joints with an extension deficit for knee and hip > 30°, open areas in the area of padding or belt supports.
Every effort was made to include all eligible patients in the study period. The inclusion of at least 30 patients was planned – at least 10 patients in each subgroup of FAC 0-2.
Therapists
All therapists included in the study had to be familiar with the settings and setup procedures, and be able to demonstrate routines in handling the gait trainer.
During measurements, only one therapist was allowed to assist the patient. A maximum of three patient run-throughs were documented per therapist.
All therapists included in the study had to be familiar with the settings and setup procedures, and be able to demonstrate routines in handling the gait trainer.
During measurements, only one therapist was allowed to assist the patient. A maximum of three patient run-throughs were documented per therapist.
Statistics
The mean values, standard errors and 95% confidence intervals of all measurement results were firstly determined. There was also a subgroup analysis, categorised by FAC and SP. As a preliminary test for inferential statistical analysis, the data was checked for normal distribution with the Shapiro-Wilk test and Kolmogorov-Smirnov test at the selected significance level of α = 5% (p = 0.05). The empirical distribution of the measurement results did not differ significantly from a normal distribution (Shapiro-Wilk: z= .959, .971; p = .242, .508; df = 33 and Kolmogorow-Smirnow: z = .094, .104; p = .200; df = 33). Both tests confirmed the assumption of a normal distribution. Assuming the null hypothesis, the mean values and standard errors of the subdomains could be examined for significant differences using a t-test for independent samples. Here, too, α = 5 % (p = 0.05) was defined as the significance level.
The statistical evaluation of the data was carried out with statistics program SPSS® Statistics for Macintosh, version 24.00.00.
Die statistische Auswertung der Daten erfolgte mit dem Statistikprogramm SPSS® Statistics für Macintosh, Version 24.00.00.
The mean values, standard errors and 95% confidence intervals of all measurement results were firstly determined. There was also a subgroup analysis, categorised by FAC and SP. As a preliminary test for inferential statistical analysis, the data was checked for normal distribution with the Shapiro-Wilk test and Kolmogorov-Smirnov test at the selected significance level of α = 5% (p = 0.05). The empirical distribution of the measurement results did not differ significantly from a normal distribution (Shapiro-Wilk: z= .959, .971; p = .242, .508; df = 33 and Kolmogorow-Smirnow: z = .094, .104; p = .200; df = 33). Both tests confirmed the assumption of a normal distribution. Assuming the null hypothesis, the mean values and standard errors of the subdomains could be examined for significant differences using a t-test for independent samples. Here, too, α = 5 % (p = 0.05) was defined as the significance level.
The statistical evaluation of the data was carried out with statistics program SPSS® Statistics for Macintosh, version 24.00.00.
Die statistische Auswertung der Daten erfolgte mit dem Statistikprogramm SPSS® Statistics für Macintosh, Version 24.00.00.
Results
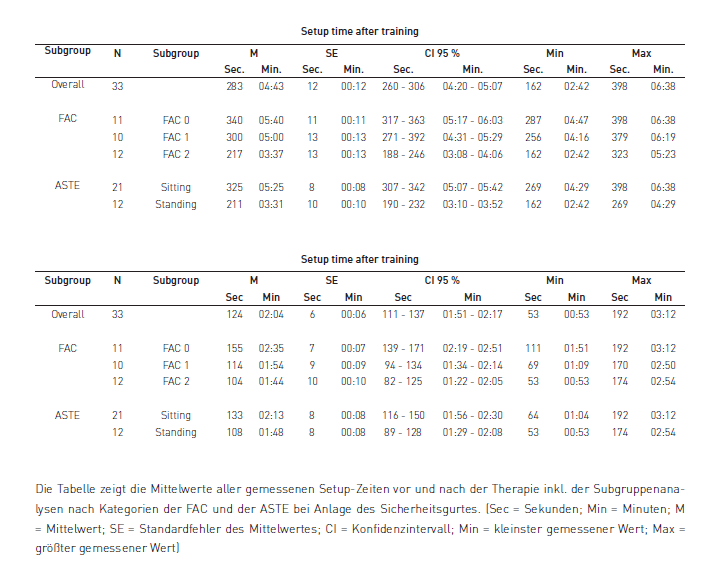
A total of 33 patients were recruited during the study period, 11 of whom were assigned to subgroup “FAC 0”, 10 to subgroup “FAC 1” and 12 to subgroup “FAC 2”. 21 of the 33 patients had the safety belt set up in the sitting position. For the remaining 12 patients, the therapist was able to set up the safety belt in the standing position.
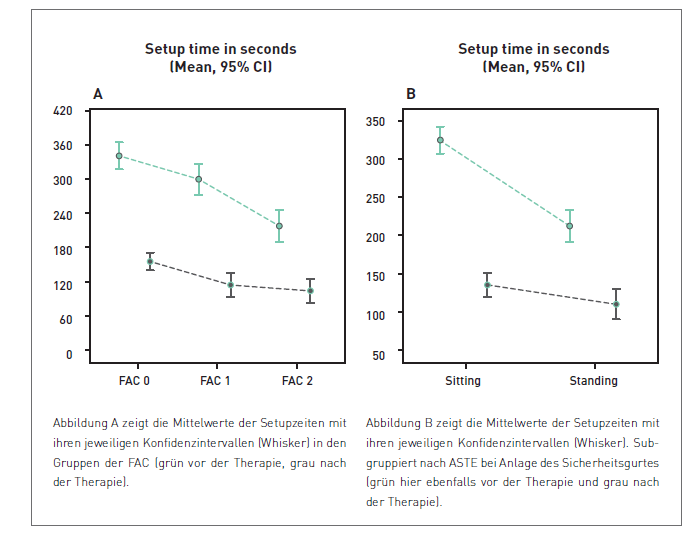
The mean setup time before therapy was 4.43 minutes (CI 95 % 4.20 – 5.07 min) and after therapy 2.04 minutes (CI 95 % 1.51 – 2.17 min).
The mean setup time before therapy for patients in patient group “FAC 0” was 5.40 minutes (CI 95 % 5.17 – 6.03 min), in group “FAC 1” 5.00 minutes (CI 95 % 4.31 – 5.29 min), and in group “FAC 2” 3.37 minutes (CI 95 % 3.08 – 4.06 min). The mean setup time after therapy in patient group “FAC 0” was 2.35 minutes (CI 95 % 2.19 – 2.51 min), in group “FAC 1” 1.54 minutes (CI 95 % 1.34 – 2.14 min), and in group “FAC 2” 1.44 minutes (CI 95 % 1.22 – 2.05 min).
The setup time in the “SP Sitting” group before therapy was 5.25 minutes on average (CI 95 % 5.07 – 5.42 min) and after therapy 2.13 minutes (CI 95 % 1.56 – 2.30 min). The setup time in the “SP Standing” group before therapy was 3.31 minutes on average (CI 95 % 3.10 – 3.52 min) and after therapy 1.48 minutes (CI 95 % 1.29 – 2.08 min).
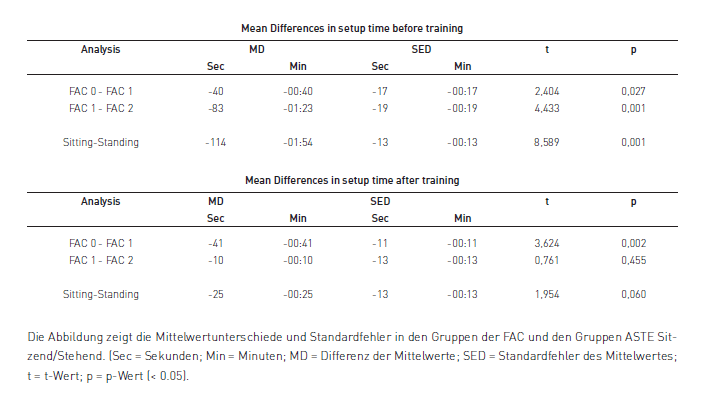
In the “FAC 1” group, the setup time before therapy was 0.40 minutes (SD 0.17 min; p = .027) shorter than the “FAC 0” group, and in the “FAC 2” group it was 1.23 minutes (SD 0.19 min; p = 0.001) shorter than the “FAC 1” group.
After therapy, the average setup time in the “FAC 1” group was 0.41 minutes (SD 0.11 min;
p = 0.002) shorter than the “FAC 2” group, and the “FAC 2” group 0.10 minutes (SD 0.13 min;
p = .455) shorter than the “FAC 1” group.
The setup time in the “SP Standing” group was on average 1.54 minutes (SD 0.13 min; p = .001) shorter before therapy and 0.25 minutes (SD 0.13 min; p = .06) shorter after therapy compared to the “SP Sitting” group.
A total of 33 patients were recruited during the study period, 11 of whom were assigned to subgroup “FAC 0”, 10 to subgroup “FAC 1” and 12 to subgroup “FAC 2”. 21 of the 33 patients had the safety belt set up in the sitting position. For the remaining 12 patients, the therapist was able to set up the safety belt in the standing position.
The mean setup time before therapy was 4.43 minutes (CI 95 % 4.20 – 5.07 min) and after therapy 2.04 minutes (CI 95 % 1.51 – 2.17 min).
The mean setup time before therapy for patients in patient group “FAC 0” was 5.40 minutes (CI 95 % 5.17 – 6.03 min), in group “FAC 1” 5.00 minutes (CI 95 % 4.31 – 5.29 min), and in group “FAC 2” 3.37 minutes (CI 95 % 3.08 – 4.06 min). The mean setup time after therapy in patient group “FAC 0” was 2.35 minutes (CI 95 % 2.19 – 2.51 min), in group “FAC 1” 1.54 minutes (CI 95 % 1.34 – 2.14 min), and in group “FAC 2” 1.44 minutes (CI 95 % 1.22 – 2.05 min).
The setup time in the “SP Sitting” group before therapy was 5.25 minutes on average (CI 95 % 5.07 – 5.42 min) and after therapy 2.13 minutes (CI 95 % 1.56 – 2.30 min). The setup time in the “SP Standing” group before therapy was 3.31 minutes on average (CI 95 % 3.10 – 3.52 min) and after therapy 1.48 minutes (CI 95 % 1.29 – 2.08 min).
In the “FAC 1” group, the setup time before therapy was 0.40 minutes (SD 0.17 min; p = .027) shorter than the “FAC 0” group, and in the “FAC 2” group it was 1.23 minutes (SD 0.19 min; p = 0.001) shorter than the “FAC 1” group.
After therapy, the average setup time in the “FAC 1” group was 0.41 minutes (SD 0.11 min;
p = 0.002) shorter than the “FAC 2” group, and the “FAC 2” group 0.10 minutes (SD 0.13 min;
p = .455) shorter than the “FAC 1” group.
The setup time in the “SP Standing” group was on average 1.54 minutes (SD 0.13 min; p = .001) shorter before therapy and 0.25 minutes (SD 0.13 min; p = .06) shorter after therapy compared to the “SP Sitting” group.
Discussion
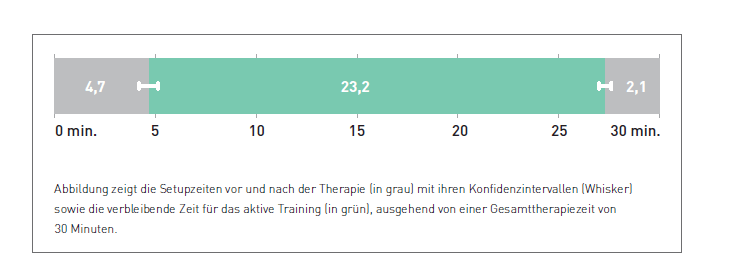
The aim of the study was to collect average setup times using the THERA-Trainer lyra as part of locomotion therapy. The results of the study show that the time required for set up and transfer is about 7 minutes on average. Based on the assumption that a gait trainer session takes an average of 30 minutes, this leaves about 23 minutes for active training in the device.
The setup time, particularly before therapy, reduces as the patient’s mobility score increases. The starting position when setting up the safety belt appears to have a particularly big impact here. Setting up the belt in the standing position reduces the setup time by about one third. This coincides with the results of qualitative surveys. Therapists confirm that setting up the safety belt in the standing position is simpler and clearly saves time.
The aim of the study was to collect average setup times using the THERA-Trainer lyra as part of locomotion therapy. The results of the study show that the time required for set up and transfer is about 7 minutes on average. Based on the assumption that a gait trainer session takes an average of 30 minutes, this leaves about 23 minutes for active training in the device.
The setup time, particularly before therapy, reduces as the patient’s mobility score increases. The starting position when setting up the safety belt appears to have a particularly big impact here. Setting up the belt in the standing position reduces the setup time by about one third. This coincides with the results of qualitative surveys. Therapists confirm that setting up the safety belt in the standing position is simpler and clearly saves time.
Implications for clinical practice
Depending on their motor skills, patients should be actively involved in preparing and following up electromechanical gait therapy. This will create the opportunity to reduce setup times in order to generate more time for active training in the device.
Depending on their motor skills, patients should be actively involved in preparing and following up electromechanical gait therapy. This will create the opportunity to reduce setup times in order to generate more time for active training in the device.
In the case of an average gait training session of 30 minutes using the lyra, approximately 23 minutes are left for active training in the device.
The safety belt should be set up in the standing position, wherever possible, because this can save the most time. Waiting times when directly changing from one patient to the next can be compensated, for example, by using several belt systems and an overlapping schedule.
Jakob Tiebel
Health Business Consultant
Jakob Tiebel is OT and studied applied psychology with a focus on health economics. He has clinical expertise from his previous therapeutic work in neurorehabilitation. He conducts research and publishes on the theory-practice transfer in neurorehabilitation and is the owner of an agency for digital health marketing.
References:
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.