TECHNOLOGY AND DEVELOPMENT
Dead end in productdevelopment
A critical look at a new in-bed prototype – and why in-bed cycling
remains a complex challenge in practice, use and regulation

Jakob Tiebel
Health Business Consultant
Early mobilisation is considered one of the most important factors in limiting loss of function, complications and dependency on care among bed-resting patients. At the same time, it is generally difficult to implement in everyday clinical practice. Time pressure, staff shortages and serious clinical pictures mean that early mobilisation is often a goal that does not easily become routine practice. Against this background, it is not surprising that new devices are constantly being developed to enable exercise therapy in bed. One current example is provided by an article in Actuators (2025) on the technical development of a prototype for an in-bed lower-limb therapy device.
The item is technically ambitious, but it raises a crucial question: Is a solution being built here that will really advance healthcare – or is a problem merely being translated into an elegant machine without considering the benefits, safety and feasibility in a real-life setting?
The item is technically ambitious, but it raises a crucial question: Is a solution being built here that will really advance healthcare – or is a problem merely being translated into an elegant machine without considering the benefits, safety and feasibility in a real-life setting?
What was developed?
The team of authors describe a compact therapy device that is used directly on a hospital bed. It consists of two motorised foot plates with integrated force sensors. Four electric motors control linear movements of the foot plates and rotation in the ankle joint. The intention here is to enable several forms of training: passive plantar flexion/dorsiflexion, passive linear leg movement with synchronised ankle joint movement and active leg press training with adjustable resistance loads. The system is controlled via a touchscreen; exergames have also been implemented to accompany movements and provide feedback.
The core technical service lies in controlling movement and force. The article reports control accuracies, for example average position deviations in the millimetre range and low force control deviations in active mode. In addition, usability is assessed using questionnaires – on healthy test subjects.
The core technical service lies in controlling movement and force. The article reports control accuracies, for example average position deviations in the millimetre range and low force control deviations in active mode. In addition, usability is assessed using questionnaires – on healthy test subjects.
Technical sophistication does not bypass the logic of care: a device is not good if it can do something, but if it can be used reliably under real clinical conditions.
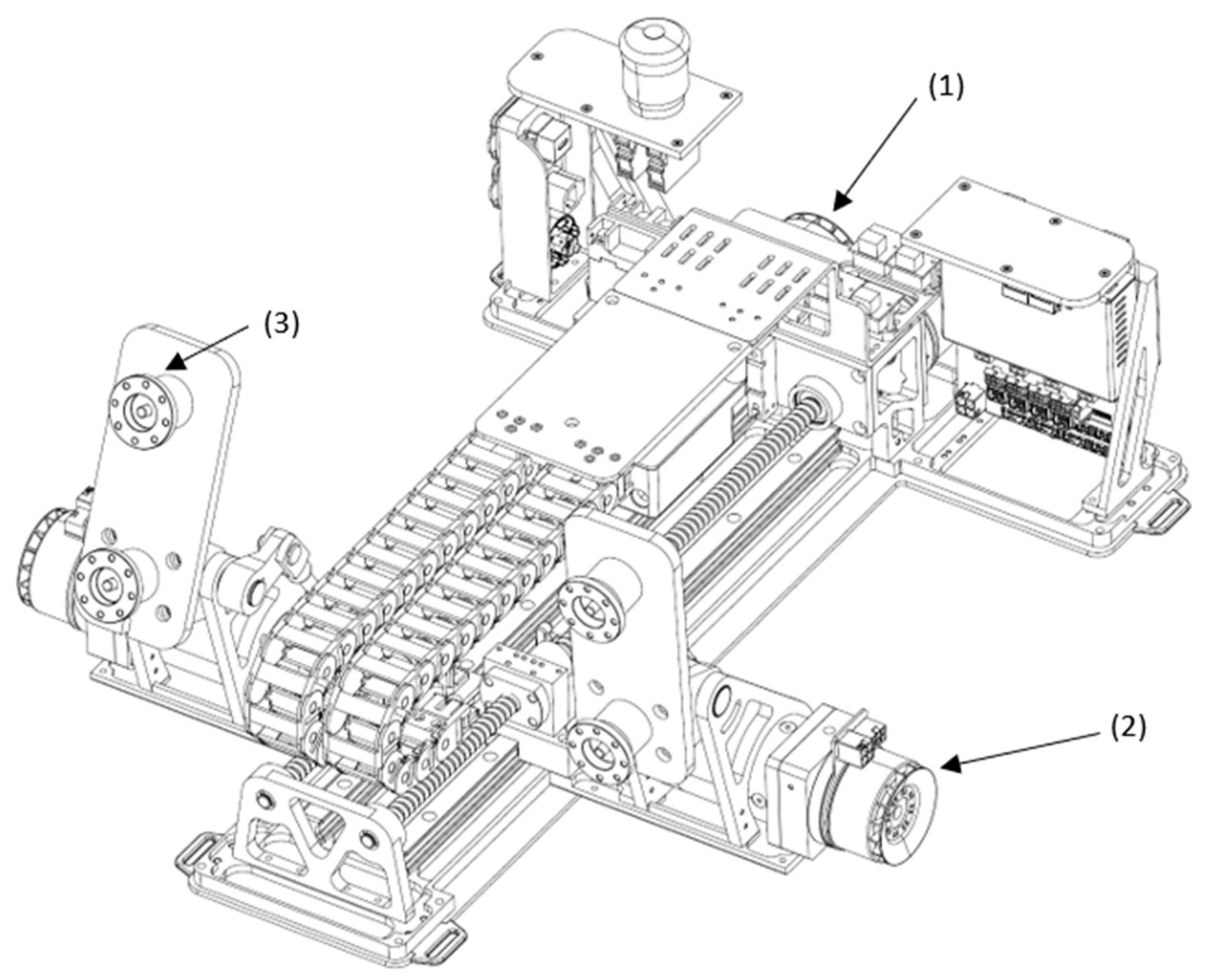
CAD of the lower-limb therapy device. The system housing, the foot plates, and the cases for the foot platforms were removed so as to show the drives and mechanical components. (1) Motor for linear movement, (2) motor for ankle dorsiflexion/plantarflexion, and (3) force sensor. – Source: Fang et al. (2025); original image taken from Open Access Publication without changes
What does the study say?
The authors state their goal clearly: they want to demonstrate the technical feasibility and usability of a prototype. And that’s exactly what they deliver. The device was tested in a laboratory setting with twelve healthy adults, who completed short test sequences in the passive and active modes. They then evaluated the device using a modified usability questionnaire. The feedback was generally positive, but there were also indications of problems that are in no way trivial in practice. At around 18 kg, the device is not really “lightweight” and therefore presents transport limitations. A delay was also perceived between real movement and exergame feedback, and basic set-up and workflow frictions were observed.What the authors explain in their publication as “technically feasible” is often intuitively equated with “relevant for early mobilisation”. This is precisely where it is worth taking a critical look.
The comparison with in-bed cycling
The article places the developed device in the early mobilisation market and draws parallels with established in-bed cycling systems such as the THERA-Trainer bemo. It is exactly here that the comparison becomes relevant: In-bed cycling has been a clinically established and effective procedure in early rehabilitation and acute care for years because it is a practicable principle for applying activity under real care conditions and has been proven to be safe and reliable.
In-bed therapy rarely fails because of motors or sensors – but because of complexity, regulation and a lack of process robustness in everyday life.
In-bed cycling generates a cyclical movement, allows for adequate dosing via assistive drive control and is easy to operate and implement. As a clearly defined medical device, a THERA-Trainer bemo can be integrated reliably, safely and quickly into existing clinical routines, for example. The critical factor here is less the degree of “high tech” than the fact that the process has been tried and tested many times, and actually works under everyday conditions. In early mobilisation, this ease of implementation weighs heavily in its favour.
In contrast, the newly developed prototype device utilises complex mechatronic axes and force sensors. While this may theoretically open up other therapeutic options, in practice it also increases the likelihood of sources of error, training requirements, maintenance needs, failure risks and process interruptions. Clinical added value and benefits would first have to be established.
In contrast, the newly developed prototype device utilises complex mechatronic axes and force sensors. While this may theoretically open up other therapeutic options, in practice it also increases the likelihood of sources of error, training requirements, maintenance needs, failure risks and process interruptions. Clinical added value and benefits would first have to be established.
Technical control and clinical safety are not one and the same
The device presented works with motorised foot plates that generate linear movement and ankle joint rotation. This actively initiates forces and paths while the patient is fixed in the supine position. This is one thing for healthy subjects in the laboratory. But it immediately poses additional safety issues for real bed-resting patients: What does this mean for spasticity, contractures, osteoporosis, painful joints, impaired communication, delirium and fluctuations in vigilance? How robust are emergency stop concepts under stress? What is done to ensure that a set-up error does not lead to shear forces, skin stress or unfavourable joint loads? The article does not address these questions because it cannot yet address them methodologically. However, they are central to later translation. At this point, in-bed cycling is still the gold standard: The movement logic is extremely gentle, the forces are typically easy to control, the clinical experience is broad, and the devices are already integrated into risk processes, hygiene and training in many hospitals.
Regulation and the coupling of two medical devices
However, the most critical aspect is not the motor or the control system – but the regulation and the system definition that is relevant to liability. The developers seem to have overlooked something very important here.

The prototype of the lower-limb therapy device on a medical bed and with a test person: (1) touch screen, (2) emergency stop, (3) foot plate, and (4) force sensor. – Source: Fang et al. (2025); original image taken from Open Access Publication without changes
Regulation and the coupling of two medical devices
The prototype is placed in the bed and used there as a de facto bed-integrated solution. A hospital bed is usually a medical device itself. As soon as another medical device is used mechanically and functionally in such a way that it is dependent on the bed as a supporting structure or is operated in conjunction with it, a constellation quickly arises that for regulatory purposes can no longer be treated as “two independent devices”. This gives rise to issues such as system compatibility, safe combination, intended use when combined, interface risks, stability in different bed geometries, risks of misuse when changing beds and chains of responsibility between manufacturers.
This is not a theoretical problem. In practice, it determines whether a device can be approved and rolled out in clinics in a scalable manner. In-bed cycling is typically more cleverly designed in this respect: It remains recognisable as an independent medical device, is positioned at the bed instead of being “married” to it and as a result, avoids many issues relating to combination, integration and liability. This self-sufficiency is precisely one key reason why the design concepts of well-known manufacturers stand out accordingly.
By contrast, if a new device implicitly requires fixation or support in the bed, or functional coordination with bed mechanisms, the regulatory complexity increases considerably. While this does not make such concepts impossible, the development and authorisation process becomes longer, more ex pensive and riskier.
This is not a theoretical problem. In practice, it determines whether a device can be approved and rolled out in clinics in a scalable manner. In-bed cycling is typically more cleverly designed in this respect: It remains recognisable as an independent medical device, is positioned at the bed instead of being “married” to it and as a result, avoids many issues relating to combination, integration and liability. This self-sufficiency is precisely one key reason why the design concepts of well-known manufacturers stand out accordingly.
By contrast, if a new device implicitly requires fixation or support in the bed, or functional coordination with bed mechanisms, the regulatory complexity increases considerably. While this does not make such concepts impossible, the development and authorisation process becomes longer, more ex pensive and riskier.
Critical assessment
The article in Actuators presents a technically well-developed idea that generally works in a laboratory setting and is perceived as operable by healthy subjects. This is a legitimate step in any early development phase. However, it falls short of demonstrating clinical benefits or competing with established in-bed cycling solutions.
When assessing the project from a strictly careoriented perspective, three central touchstones remain open. Firstly, the clinical relevance, i.e. whether the training modes actually contribute to outcomes that measurably promote early mobilisation. Secondly, safety in the target group, i.e. in vulnerable patient populations with high variability. Thirdly, the regulatory and practical feasibility of implementation, particularly with regard to coupling with the hospital bed as a medical device.
Until these points are clarified, the device is more of an example of how easy it is to confuse “technically feasible” with “clinically useful”. This is a dangerous shortcut for healthcare provision. Early mobilisation needs devices that not only generate movement, but also simplify processes, reduce risks and fit neatly into realworld care from a regulatory perspective. Inbed cycling is therefore not old school, but often simply the more robust design when it comes to service delivery.
If one key insight can be derived from this development, then perhaps it is precisely this lesson: In early mobilisation, it is not the device with the most axes that wins, but the system that works safely, quickly, reliably and legally correctly under staff shortages – and supports the journey out of bed instead of being perfected in bed.
When assessing the project from a strictly careoriented perspective, three central touchstones remain open. Firstly, the clinical relevance, i.e. whether the training modes actually contribute to outcomes that measurably promote early mobilisation. Secondly, safety in the target group, i.e. in vulnerable patient populations with high variability. Thirdly, the regulatory and practical feasibility of implementation, particularly with regard to coupling with the hospital bed as a medical device.
Until these points are clarified, the device is more of an example of how easy it is to confuse “technically feasible” with “clinically useful”. This is a dangerous shortcut for healthcare provision. Early mobilisation needs devices that not only generate movement, but also simplify processes, reduce risks and fit neatly into realworld care from a regulatory perspective. Inbed cycling is therefore not old school, but often simply the more robust design when it comes to service delivery.
If one key insight can be derived from this development, then perhaps it is precisely this lesson: In early mobilisation, it is not the device with the most axes that wins, but the system that works safely, quickly, reliably and legally correctly under staff shortages – and supports the journey out of bed instead of being perfected in bed.
Jakob Tiebel
Health Business Consultant
Jakob Tiebel is OT and studied applied psychology with a focus on health economics. He has clinical expertise from his previous therapeutic work in neurorehabilitation. He conducts research and publishes on the theory-practice transfer in neurorehabilitation and is the owner of an agency for digital health marketing.
References:
- Fang, J., Cerrito, A., Gamero Schertenleib, S., von Raumer, P., & Schmitt, K.-U. (2025). The Technical Development of a Prototype Lower-Limb Therapy Device for Bed-Resting Users. Actuators, 14(2), 60. https://doi.org/10.3390/act14020060
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.