
Science
Tried and tested
Why exercise is essential for patients with chronic kidney disease

Isabelle Balge
Employee in the New Business Development, THERA-Trainer
Reducing cardiovascular morbidity and mortality in chronic kidney disease (CKD) is increasingly becoming a joint priority for both cardiology and nephrology specialists. A recent Clinical Consensus Statement from cardiology and nephrology associations highlights the essential role of exercise training in reducing cardiovascular risk in patients with CKD G3–G5D (cf. Kouidi et al. 2024).
Background
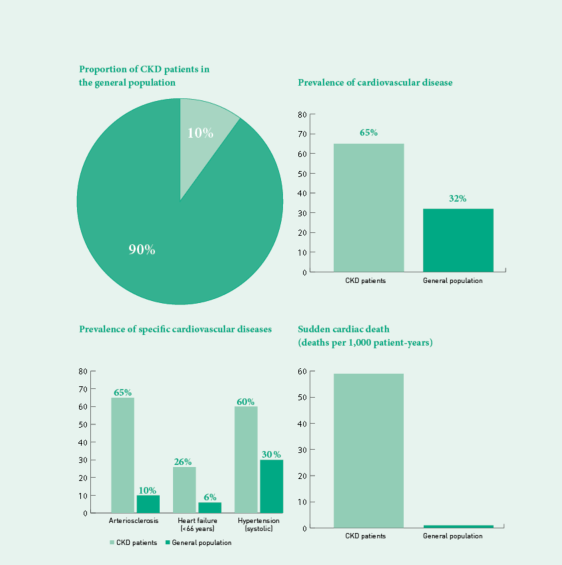
Chronic kidney disease (CKD) affects approximately 10% of the global population. Classification is based on the glomerular filtration rate (GFR), which indicates how well the kidneys filter the blood:
Stage G3: mild to moderate reduction (GFR 30–59 ml/min)
Stage G4: severe reduction (GFR 15–29 ml/min)
Stage G5: kidney failure (GFR unter 15 ml/min)
G5D: kidney failure requiring dialysis.
Background
Chronic kidney disease (CKD) affects approximately 10% of the global population. Classification is based on the glomerular filtration rate (GFR), which indicates how well the kidneys filter the blood:
Stage G3: mild to moderate reduction (GFR 30–59 ml/min)
Stage G4: severe reduction (GFR 15–29 ml/min)
Stage G5: kidney failure (GFR unter 15 ml/min)
G5D: kidney failure requiring dialysis.
Link between CKD and cardiovascular diseases
There is a close link between CKD and cardiovascular disease (CVD). Contributing factors include chronic volume overload, inflammatory processes and mineral imbalances that can increase arterial stiffness and lead to arteriosclerosis. The prevalence of arteriosclerosis is up to 65% in haemodialysis patients, while approximately 60% of peritoneal dialysis patients and individuals with CKD G3 G4 are affected.
Approximately half of patients with CKD G4–G5 suffer from CVD. They have twice as high a prevalence of cardiovascular diseases compared to the general population (65% vs 32%). Heart failure occurs significantly more frequently in CKD patients over 66 years of age (26% vs 6%), in dialysis patients the prevalence is even as high as 44%. Furthermore, the risk of sudden cardiac death in dialysis patients is markedly increased compared to the general population (59 vs 1 death per 1,000 patient-years).
Approximately half of patients with CKD G4–G5 suffer from CVD. They have twice as high a prevalence of cardiovascular diseases compared to the general population (65% vs 32%). Heart failure occurs significantly more frequently in CKD patients over 66 years of age (26% vs 6%), in dialysis patients the prevalence is even as high as 44%. Furthermore, the risk of sudden cardiac death in dialysis patients is markedly increased compared to the general population (59 vs 1 death per 1,000 patient-years).
Exercise as non-pharmacological therapy
The prevention of CVD is an important approach to improving life expectancy in CKD patients. The Clinical Consensus Statement therefore focuses on non-pharmacological therapies, particularly exercise training.
Physical activity and CKD
There is a dose-response relationship between physical activity and CKD risk, as well as overall mortality. Some studies show that physical activity can slow the progression of CKD and reduce albuminuria (protein excretion in the urine). It is estimated that CKD risk can be reduced by 2% per 10 MET-h/week.
MET-h/week describes the energy expenditure through physical activity
An increase in physical activity in CKD patients without renal replacement therapy can also improve risk factors such as hypertension and reduce cardiovascular mortality in dialysis patients. Several studies have shown that patients who are more physically active have a lower mortality rate.
Research evidence on exercise training
The DiaTT study showed that training during dialysis is safe and brings clinical benefits in patients with different comorbidities and age groups. Physical function improved, the number of hospital admissions was reduced and the hospitalisation rate was halved.
Further studies such as RENEXC and AWARD also showed positive effects on the fitness of patients with CKD G3-G5. The CYCLE-HD study reported improvements in cardiac parameters following six months of intradialytic cycle training.
Further studies such as RENEXC and AWARD also showed positive effects on the fitness of patients with CKD G3-G5. The CYCLE-HD study reported improvements in cardiac parameters following six months of intradialytic cycle training.
Traditional cardiovascular risk factors in CKD
The development of hypertension and CKD is closely interrelated. Hypertension is one of the main causes of CKD as it damages the small vessels of the kidney. Conversely, CKD promotes the development of hypertension through increased sympathetic tone and activation of the renin-angiotensin-aldosterone system. The prevalence of hypertension in CKD patients is high: 60% for systolic and 30% for diastolic blood pressure.
CKD and heart failure are closely linked pathophysiologically as cardiorenal syndrome. Both diseases share common underlying mechanisms: systemic inflammation, endothelial dysfunction and oxidative stress.
Dialysis itself poses a risk for sudden cardiac death. Possible mechanisms are insufficient dialysis dose, cardiac arrhythmias as a result of volume overload or depletion, and electrolyte imbalances during and after dialysis.
CKD and heart failure are closely linked pathophysiologically as cardiorenal syndrome. Both diseases share common underlying mechanisms: systemic inflammation, endothelial dysfunction and oxidative stress.
Dialysis itself poses a risk for sudden cardiac death. Possible mechanisms are insufficient dialysis dose, cardiac arrhythmias as a result of volume overload or depletion, and electrolyte imbalances during and after dialysis.
Fewer heart attacks, fewer hospital stays – better quality of life through exercise training.
Safety of exercise training
Exercise during dialysis is fundamentally safe when it is properly dosed. In the first two hours of dialysis, hardly any side effects occur. In cases of high ultrafiltration volumes and a risk of intradialytic hypotension, training should however be postponed until circulatory values have stabilised.
Recommendations for exercise training and conclusion
The KDIGO guidelines recommend at least 150 minutes of moderate physical activity per week. Ideally, 7,000 to 10,000 steps per day would be optimal – however, most patients do not achieve these levels.
The evidence underscores that targeted exercise training offers CKD patients numerous benefits and can be performed safely. Training should be personalised. The introduction of structured exercise programmes could be crucial in reducing cardiovascular morbidity and mortality in this high-risk group and should therefore be promoted as an integral component of CKD treatment.
The evidence underscores that targeted exercise training offers CKD patients numerous benefits and can be performed safely. Training should be personalised. The introduction of structured exercise programmes could be crucial in reducing cardiovascular morbidity and mortality in this high-risk group and should therefore be promoted as an integral component of CKD treatment.
Ambulante Rehabilitation
Cycling
Fachkreise
Produkte
Science
Stationäre Rehabilitation
THERAPY
THERAPY 2025-II
THERAPY Magazine
Wohnen im Alter & Langzeitpflege
Isabelle Balge
Employee in the New Business Development, THERA-Trainer
Isabelle Balge has several years of practical experience in the emergency medical services. Following her dual study programme in Business Administration specialising in Health Management, she has been part of THERA-Trainer’s New Business Development team since 2023. Her role includes that of Medical Liaison specialising in nephrology and dialysis. She is currently studying on a part-time basis for a master’s degree in Health Economics and Management.
References:
- Kouidi E, Hanssen H, Anding-Rost K, Cupisti A, Deligiannis A, Grupp C, Koufaki P, Leeson P, Segura-Orti E, Van Craenenbroeck A, Van Craenenbroeck E, Clyne N, Halle M. The role of exercise training on cardiovascular risk factors and heart disease in patients with chronic kidney disease G3-G5 and G5D: a Clinical Consensus Statement of the European Association of Preventive Cardiology of the ESC and the European Association of Rehabilitation in Chronic Kidney Disease. Eur J Prev Cardiol. 2024 Sep 6;31(12):1493-1515. doi: 10.1093/eurjpc/zwae130. PMID: 38593202. https://pubmed.ncbi.nlm.nih.gov/38593202/