
SCIENCE
Early end-effectorbased gait trainingin severely affectedstroke patientswith neglect
What the study shows – and what this means for the use of the lyra end-effector gait trainer

Jakob Tiebel
Health Business Consultant
Guidelines consider early, intensive gait rehabilitation to be a central component of stroke rehabilitation, especially for patients who are not yet able to walk in the subacute phase. At the same time, there is one patient group that has traditionally been underrepresented or explicitly excluded in robotic-assisted studies: people with visuospatial neglect (VSN), typically after a right-hemispheric stroke. VSN is a negative predictor of functional outcomes and makes the process of recovering mobility more difficult, among other things due to attention and perception deficits, and a lack of insight into one’s own impairments. The randomised study by Gorsler et al. addresses this evidence gap. (Frontiers in Neurology, 2025).
Question and hypothesis
The authors investigated whether early end-effector-based gait training as an addition to standard therapy in severely affected, non-ambulatory subacute stroke patients with VSN is more effective than an active control intervention (early verticalisation in a standing frame) – in each case in addition to the usual physiotherapy and neglect therapy. The primary endpoint was walking ability, while trunk stability and balance were considered secondarily.
study design, population and interventions
This is a prospective, randomised, assessor-blinded controlled study (proof-of-concept). The study included 43 patients in the early subacute phase (7–80 days post-stroke) with a first right-hemispheric stroke and left-sided VSN. All of them were non-ambulatory (FAC ≤ 2) and had to be haemodynamically stable when standing. The cohort was severely affected from a clinical standpoint (including high functional dependence, impaired trunk function).
The additional intervention consisted of nine sessions, each lasting 30 minutes, and took place over approximately two to three weeks. In the control group, patients were verticalised early in the standing frame, while in the intervention group they received end-effector-based gait training. Both groups used devices from the same manufacturer: the THERA-Trainer balo as a standing frame andthe THERA-Trainer lyra for gait training. A walking speed of at least 1.5 km/h was planned for the gait training. The body weight support (BWS) was a maximum of 30% at the beginning. If patients were clinically observed to be overwhelmed, the BWS could be temporarily increased to 60%; thereafter, the speed was reduced. This makes the study very practical: the parameters were consistently adapted to the resilience of the severely affected patients (feasibility first).
Neglect is not a reason to postpone gait training – but a reason to make it possible in a targeted manner.
Outcomes and evaluation
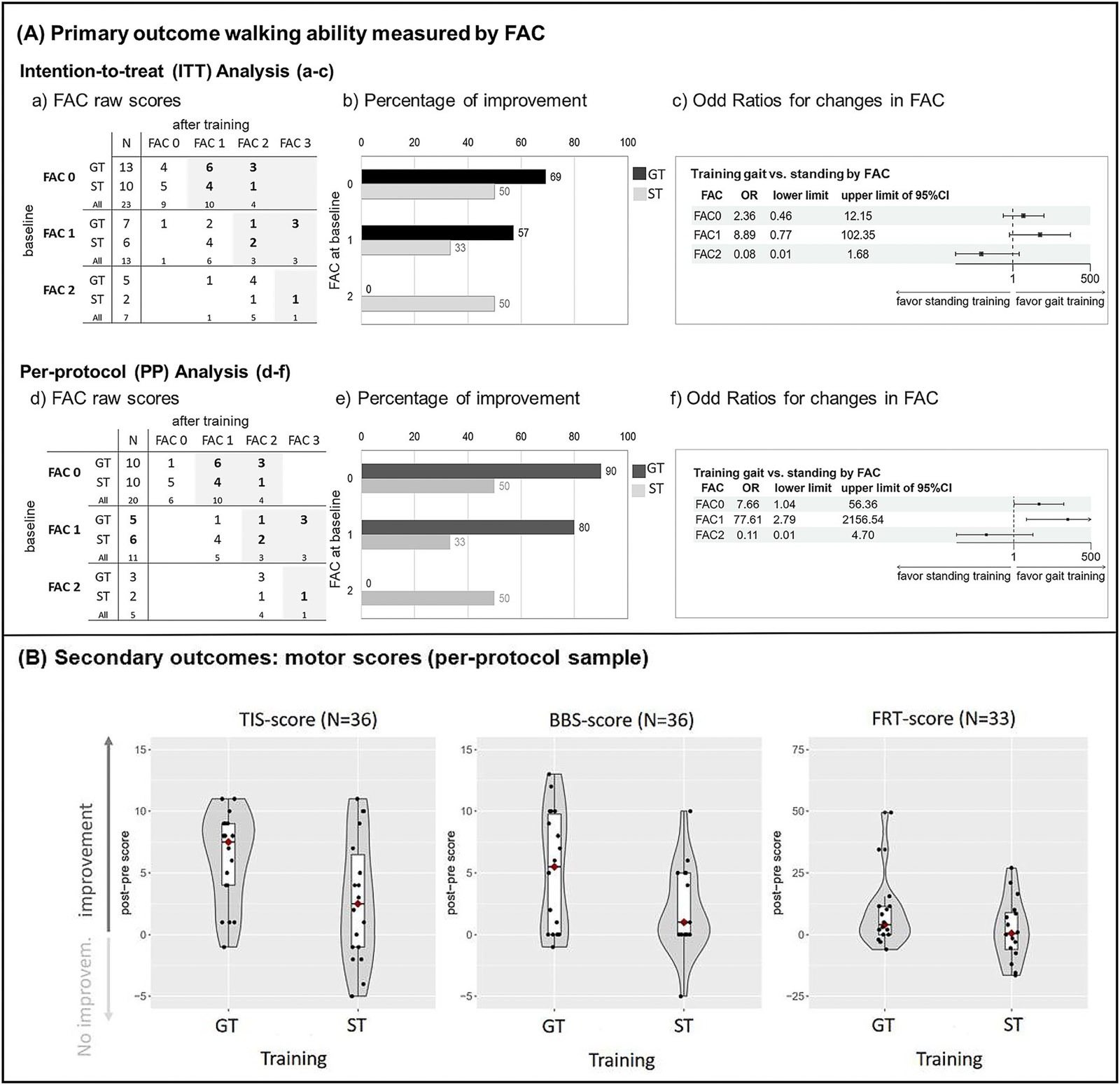
The primary outcome was the Functional Ambulation Category (FAC), analysed using ordinal logistic regression. An intention-to-treat (ITT) analysis with multiple imputation and additionally a per-protocol (PP) sensitivity analysis was performed (PP: at least 6 of 9 sessions and post-measurement).
During the intention-to-treat (ITT) analysis, all participants were analysed as they were originally assigned to the group – even if someone did not complete all the training sessions or dropped out prematurely. Missing measured values (e.g. because the final measurement is missing) were not simply omitted, but rather plausibly supplemented using a statistical method (multiple imputation). This can be pictured as follows: The programme generates multiple realistic “substitute values” based on the available data, performs calculations using these values and consolidates the results. This means that the result is less distorted than if only the “finished” cases are considered. In addition, the per-protocol (PP) analysis was carried out as a control calculation. Only those who received the treatment largely as planned were included here – in this study: at least 6 out of 9 sessions and a final measurement. This indicates whether the results are also similar when only looking at those who actually completed the programme to a sufficient extent. ITT thus marks the effect under “clinically realistic” conditions (including failures), while PP checks whether the result remains stable compared to “optimal participation”.
Secondary outcomes included the Trunk Impairment Scale (TIS) and a short form of the Berg Balance Scale (BBS).
During the intention-to-treat (ITT) analysis, all participants were analysed as they were originally assigned to the group – even if someone did not complete all the training sessions or dropped out prematurely. Missing measured values (e.g. because the final measurement is missing) were not simply omitted, but rather plausibly supplemented using a statistical method (multiple imputation). This can be pictured as follows: The programme generates multiple realistic “substitute values” based on the available data, performs calculations using these values and consolidates the results. This means that the result is less distorted than if only the “finished” cases are considered. In addition, the per-protocol (PP) analysis was carried out as a control calculation. Only those who received the treatment largely as planned were included here – in this study: at least 6 out of 9 sessions and a final measurement. This indicates whether the results are also similar when only looking at those who actually completed the programme to a sufficient extent. ITT thus marks the effect under “clinically realistic” conditions (including failures), while PP checks whether the result remains stable compared to “optimal participation”.
Secondary outcomes included the Trunk Impairment Scale (TIS) and a short form of the Berg Balance Scale (BBS).
Those most severely affected in particular benefit not only from standing, but also from early, task-oriented walking.
Primary results: Comparison of gait training vs standing training at the main endpoint (walking ability/FAC)
The ITT analysis showed no statistically significant superiority of the end-effector-based gait training over the standing frame control measure (OR 1.20; 95% CI 0.30–4.78). The overall superiority was also not significant in the PP analysis (OR 4.08; 95% CI 0.80–20.87), but with a significantly larger effect size and broad uncertainty (confidence interval), as is typical for small proof-of-concept studies.
The critical factor is the interaction effect identified by the authors. The PP analysis showed a pattern by which patients with very low initial walking ability (FAC 0–1, i.e. completely unable to walk or only able to walk with substantial manual assistance) were more likely to benefit from gait training than from standing training. Patients with FAC 2 did not display this pattern, which the authors also attribute to having very small subgroups. In practical terms, this means that the results speak less in favour of a one-sizefits-all effect and more in favour of a subgroup effect in very severely affected people, who have often not been considered in research to date.
Another finding pertinent to dosage and implementation was the positive correlation between the number of completed training sessions and FAC improvement. This supports the clinical intuition that adherence and sustained exposure are central in this population – and explains why PP analyses may be more informative here than pure ITT estimates.
The critical factor is the interaction effect identified by the authors. The PP analysis showed a pattern by which patients with very low initial walking ability (FAC 0–1, i.e. completely unable to walk or only able to walk with substantial manual assistance) were more likely to benefit from gait training than from standing training. Patients with FAC 2 did not display this pattern, which the authors also attribute to having very small subgroups. In practical terms, this means that the results speak less in favour of a one-sizefits-all effect and more in favour of a subgroup effect in very severely affected people, who have often not been considered in research to date.
Another finding pertinent to dosage and implementation was the positive correlation between the number of completed training sessions and FAC improvement. This supports the clinical intuition that adherence and sustained exposure are central in this population – and explains why PP analyses may be more informative here than pure ITT estimates.
Secondary results:Accompanying secondary endpoints (trunk, balance) and neglect/SVV
While the primary endpoint was not formally significant, the secondary outcomes showed a much clearer picture: greater improvements in trunk function (TIS; mean difference 3.4 points [95% CI 0.8–6.1], partial η² = 0.18) and balance (BBS; 5.7 points [0.5–6.7], partial η² = 0.15) were reported after gait training than after standing training. In contrast, the ability to lean forward while sitting (FRT sitting) differed only slightly between the groups (4.0 cm [-0.2–17.3], partial η² = 0.12).
The MCID-related findings (Minimal Clinically Important Difference) are particularly convincing because they translate the statistical effects into clinically relevant improvements. For TIS (MCID = 3 points), 78% of patients in the gait training group achieved a clinically relevant improvement, compared to 33% in the standing training group. For the BBS (MCID = 6-7 points), this figure was 50% after gait training versus 11% after standing training. Clinically relevant changes occurred with similar frequency during FRT in a sitting position (MCID = 6 cm) (gait training 41%, standing training 38%). Functionally, this pattern is plausible because end-effector-based training not only generates verticalisation and orthostatic activation, but also repetitive, task-oriented weight shifting, rhythmic leg movement and coordinative demands that specifically address trunk control and balance in the direction of standing/walking. It is important to mention that the neglect symptoms themselves and the subjective visual vertical (SVV) improved similarly in both groups; gait training therefore had no negative influence on neglect recovery, but also showed no specific additional benefit for this.
The MCID-related findings (Minimal Clinically Important Difference) are particularly convincing because they translate the statistical effects into clinically relevant improvements. For TIS (MCID = 3 points), 78% of patients in the gait training group achieved a clinically relevant improvement, compared to 33% in the standing training group. For the BBS (MCID = 6-7 points), this figure was 50% after gait training versus 11% after standing training. Clinically relevant changes occurred with similar frequency during FRT in a sitting position (MCID = 6 cm) (gait training 41%, standing training 38%). Functionally, this pattern is plausible because end-effector-based training not only generates verticalisation and orthostatic activation, but also repetitive, task-oriented weight shifting, rhythmic leg movement and coordinative demands that specifically address trunk control and balance in the direction of standing/walking. It is important to mention that the neglect symptoms themselves and the subjective visual vertical (SVV) improved similarly in both groups; gait training therefore had no negative influence on neglect recovery, but also showed no specific additional benefit for this.
If walking ability is not yet achievable, trunk and balance become the critical lever in rehabilitation.
Safety and compatibility
The study reports isolated training dropouts in the gait training group in connection with pain (in the case of pre-existing knee pain) or cardiac exercise intolerance in the case of pre-existing illnesses. No other adverse events were reported; affected patients were always able to continue routine therapy. In practice, the message is clear: in this multimorbid, severely affected cohort, systematic screening, close monitoring (e.g. oxygenation, pain, orthostasis) and adaptive parameter management are essential. This fits with the real-world observation of the study that the originally planned minimum speed was initially not achievable in many cases and the average BWS was above the recorded target limit – important information for protocol design and clinical pathways.
Benefit argumentation with a focus on the end-effector gait trainer
Neglect is not a reason for exclusion from early gait training
The study’s key scientific achievement is that it examines a patient group that has been excluded from many robotic/device-assisted gait training studies. In doing so, it provides proof of feasibility and initial evidence of the effectiveness of end-effector-based training in VSN. For clinics, this means that in principle, early device-assisted, task-specific gait training can also be implemented in neglect, provided that the right general conditions (vigilance, orthostasis stability, contraindications) are in place.
The study’s key scientific achievement is that it examines a patient group that has been excluded from many robotic/device-assisted gait training studies. In doing so, it provides proof of feasibility and initial evidence of the effectiveness of end-effector-based training in VSN. For clinics, this means that in principle, early device-assisted, task-specific gait training can also be implemented in neglect, provided that the right general conditions (vigilance, orthostasis stability, contraindications) are in place.
Trunk control and balance as enablers
Especially in early rehabilitation and the severe subacute phase, walking ability is often a late outcome. Improvements in trunk stability and balance, meanwhile, are often earlier, highly relevant intermediate goals in therapy because they influence transfers, sitting/standing tolerance, preparation for standing and walking, and ultimately the intensity of rehabilitation. The stronger secondary effects on TIS and BBS suggest that gait training in this cohort can act as functional priming – and is therefore clinically valuable even if a global FAC difference does not (yet) become significant in the short term.
Especially in early rehabilitation and the severe subacute phase, walking ability is often a late outcome. Improvements in trunk stability and balance, meanwhile, are often earlier, highly relevant intermediate goals in therapy because they influence transfers, sitting/standing tolerance, preparation for standing and walking, and ultimately the intensity of rehabilitation. The stronger secondary effects on TIS and BBS suggest that gait training in this cohort can act as functional priming – and is therefore clinically valuable even if a global FAC difference does not (yet) become significant in the short term.
Added value, especially for very severely affected patients (FAC 0–1)
The PP pattern suggests that patients with very low baseline FAC in particular benefit from end-effector-based training. This is clinically significant because this group is often most at risk of getting “stuck” in passive verticalisation or preparatory formats. Electromechanical gait training offers a structured way of training repetitive, task-related gait components at a very early stage – with adaptive BWS and customised dosing. The study does not provide definitive confirmation of effectiveness, but it does provide a plausible signal.
The PP pattern suggests that patients with very low baseline FAC in particular benefit from end-effector-based training. This is clinically significant because this group is often most at risk of getting “stuck” in passive verticalisation or preparatory formats. Electromechanical gait training offers a structured way of training repetitive, task-related gait components at a very early stage – with adaptive BWS and customised dosing. The study does not provide definitive confirmation of effectiveness, but it does provide a plausible signal.
Progressive protocol instead of rigid target parameters
The fact that the target speed was often not achieved initially and that BWS had to be increased more frequently is not a failure, but a realistic implementation finding. A stringent conclusion can be drawn from this for the clinical use of the lyra end-effector trainer: protocols should be planned progressively (e.g. start with higher BWS/lower speed, clear progression criteria, close symptom monitoring) instead of starting with best-practice parameters from less severely affected cohorts.
The fact that the target speed was often not achieved initially and that BWS had to be increased more frequently is not a failure, but a realistic implementation finding. A stringent conclusion can be drawn from this for the clinical use of the lyra end-effector trainer: protocols should be planned progressively (e.g. start with higher BWS/lower speed, clear progression criteria, close symptom monitoring) instead of starting with best-practice parameters from less severely affected cohorts.
Limitations
The authors emphasise the small sample size, dropouts (exclusively in the gait training group) and lack of long-term follow-up. Accordingly, the study should primarily be read as a proof of concept with hypothesis generation. It demonstrates feasibility and provides evidence of potential subgroup effects and secondary functional gains, but does not provide a conclusive efficacy assessment for all VSN patients
Conclusion
The study suggests that early end-effector-based gait training with the THERA-Trainer lyra is feasible in severely affected, non-ambulatory subacute stroke patients with visuospatial neglect and can offer clinically relevant advantages over pure verticalisation, especially in very severely affected patients and with regard to trunk stability and balance – provided that an adaptive, safety-conscious training and monitoring setting is used.
Jakob Tiebel
Health Business Consultant
Jakob Tiebel is OT and studied applied psychology with a focus on health economics. He has clinical expertise from his previous therapeutic work in neurorehabilitation. He conducts research and publishes on the theory-practice transfer in neurorehabilitation and is the owner of an agency for digital health marketing.
References:
- Gorsler A, Ernst D, Grittner U, Harnack D, Koßmehl P, Mehrholz J, Mueske C, Schneider P and Kuelzow N (2025) Early end-effector based gait training in non-ambulatory patients with visuospatial neglect after subacute stroke. Front. Neurol. 16:1639659. doi: 10.3389/fneur.2025.1639659 https://www.frontiersin.org/journals/neurology/articles/10.3389/ fneur.2025.1639659/full
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.