TECHNOLOGY & DEVELOPMENT
Connected assistance systems in outpatient fall prevention
Evidence from CARE REGIO and the role of the THERA-Trainer

Jakob Tiebel
Health Business Consultant
What happens when digital fall prevention doesn’t stop at data collection? The CARE REGIO study indicates that the actual added value of care does not lie in individual sensors, but in the intelligent combination of monitoring, suitability for everyday use and exercise-based intervention. This brings a central question into focus: Under what conditions can digital assistance systems be embedded in outpatient care in such a way that they not only promise safety, but actually counteract functional decline – and transform fall prevention from a technical add-on into an effective care mandate?
Fall prevention as a care mandate
Outpatient care for elderly people in German-speaking countries is under twofold pressure to transform. On the one hand, the demographic change is leading to an increasing proportion of very elderly people with multimorbidity and functional limitations; on the other hand, the shortage of skilled labour in care and therapy is worsening. Falls are a key risk event in this setting, as they often mark the threshold from fragile independence to acute hospitalisation, functional decline and permanent need for care. Preventive strategies that can be integrated into the everyday lives of those affected and at the same time support care and therapeutic processes are therefore highly relevant.
Digital assistance systems have been discussed for years as a potential lever for strengthening prevention, monitoring and care coordination in home contexts. Nevertheless, translation into
routine care remains limited. One key cause of this is not so much the availability of individual devices as their lack of integration into work processes, insufficient user-friendliness and a lack of support with implementation and operation. Against this background, the study “Digital assistants for outpatient care: benefits of intelligent connected assistive systems for caregivers and elderly people” (Gaßner et al., 2025) conducted in the CARE REGIO context addresses the question of whether a holistic, connected combination of assistance technologies in outpatient fall prevention generates a measurable and subjectively perceptible additional benefit – and under what conditions this benefit can be realised.
Digital assistance systems have been discussed for years as a potential lever for strengthening prevention, monitoring and care coordination in home contexts. Nevertheless, translation into
routine care remains limited. One key cause of this is not so much the availability of individual devices as their lack of integration into work processes, insufficient user-friendliness and a lack of support with implementation and operation. Against this background, the study “Digital assistants for outpatient care: benefits of intelligent connected assistive systems for caregivers and elderly people” (Gaßner et al., 2025) conducted in the CARE REGIO context addresses the question of whether a holistic, connected combination of assistance technologies in outpatient fall prevention generates a measurable and subjectively perceptible additional benefit – and under what conditions this benefit can be realised.
Mixed-methods study in a real-world home setting
The study follows a mixed-methods design that combines qualitative interviews with quantitative questionnaire surveys. The approach is explorative and clearly focussed on real-world care practice: care recipients used the systems in their own homes for five weeks; caregivers accessed the resulting data via a data integration platform. The central idea was to create a connected assistive system: vital parameter and activity data is collected via various devices, collated interoperably and made available for use by caregivers.
Participants
A total of 33 people took part: 11 caregivers and 22 care recipients. The average age of the care recipients was 80.7 years (range 54–95 years). The caregivers were on average 45.6 years old, with an average of around 19 years of work experience. Inclusion criteria for care recipients included the ability to use the systems independently; people with considerable difficulties in handling technology or with a transition to inpatient care were excluded
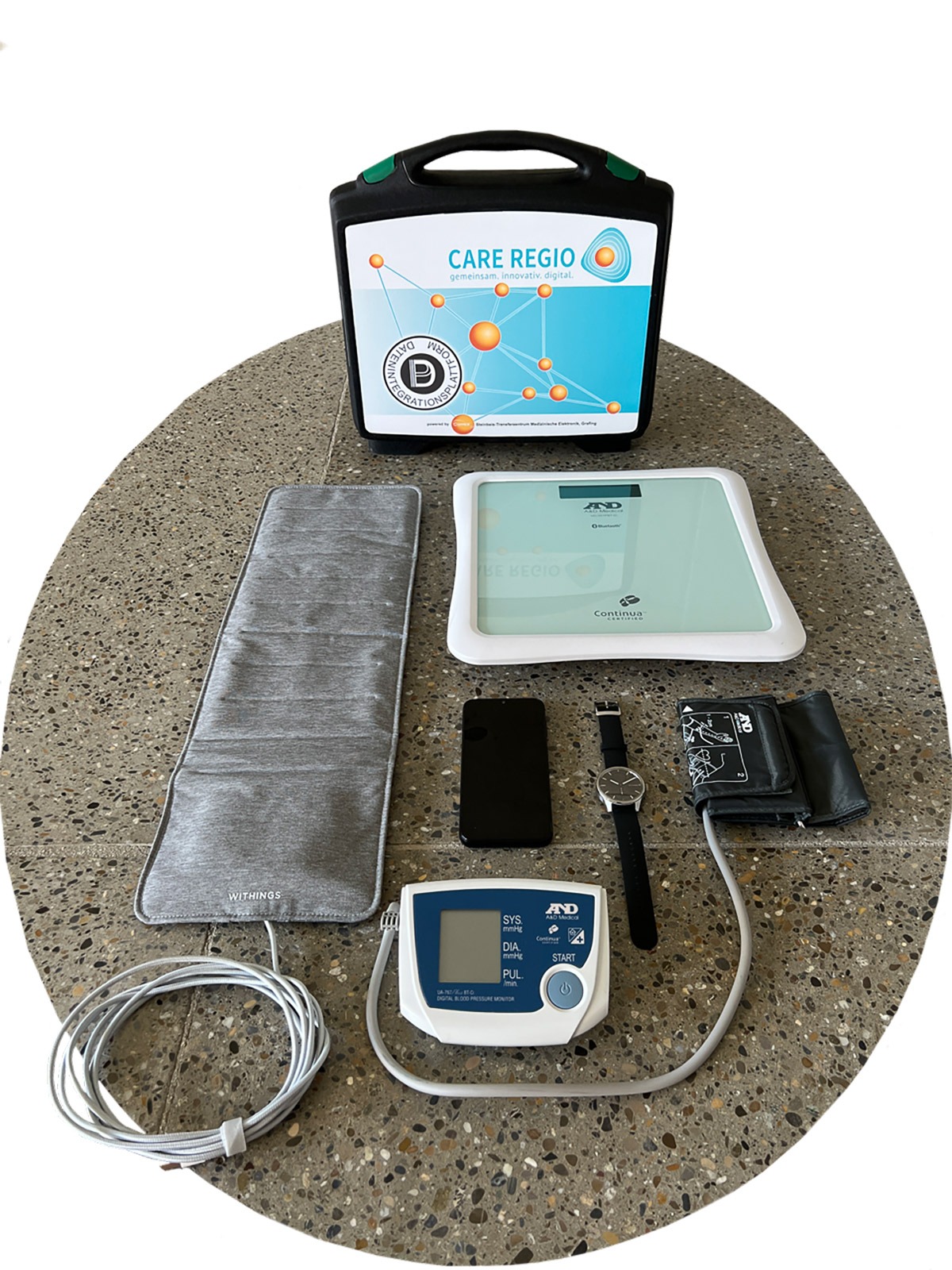
Assistive systems
The selection was needs-based: care recipients were able to choose up to five systems together with the caregivers. These included a smartwatch (Withings ScanWatch 2), a sleep mat (Withings Sleep Analyzer), a blood pressure monitor and scales (A&D), as well as a leg trainer, the THERA-Trainer tigo, as an exercise-related intervention.
Participants
A total of 33 people took part: 11 caregivers and 22 care recipients. The average age of the care recipients was 80.7 years (range 54–95 years). The caregivers were on average 45.6 years old, with an average of around 19 years of work experience. Inclusion criteria for care recipients included the ability to use the systems independently; people with considerable difficulties in handling technology or with a transition to inpatient care were excluded
Assistive systems
The selection was needs-based: care recipients were able to choose up to five systems together with the caregivers. These included a smartwatch (Withings ScanWatch 2), a sleep mat (Withings Sleep Analyzer), a blood pressure monitor and scales (A&D), as well as a leg trainer, the THERA-Trainer tigo, as an exercise-related intervention.

Fall prevention does not start with the fall – but with daily movement in everyday life.
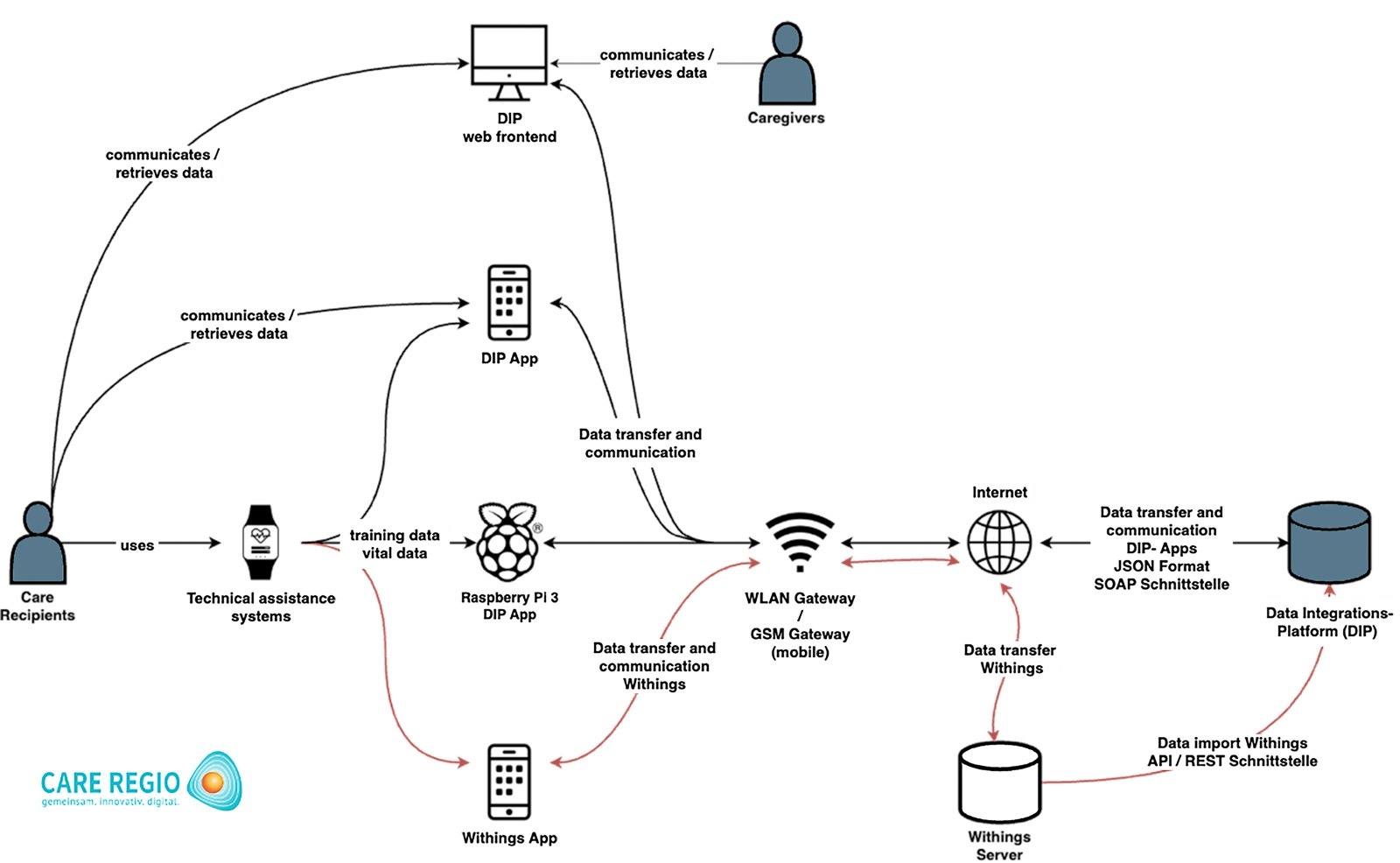
Data integration
The data integration platform (DIP) was based on the COMES® telemedicine system and was further developed with additional middleware and a new web front end for caregivers. The study explicitly emphasises that deficits in interoperability and transmission stability had been identified in earlier field tests and were specifically addressed before the start of the study – a relevant step, as technical reliability is a prerequisite for any implementation of care.
Survey instruments
Qualitative interviews were conducted before and after the intervention and analysed using Mayring’s structured content analysis. Quantitatively, the system usability scale (SUS) was used for care recipients; for carers, a specially developed questionnaire about integration into routine and perceived usefulness was used. In addition, technical stability was assessed indirectly via documented service interventions.
The data integration platform (DIP) was based on the COMES® telemedicine system and was further developed with additional middleware and a new web front end for caregivers. The study explicitly emphasises that deficits in interoperability and transmission stability had been identified in earlier field tests and were specifically addressed before the start of the study – a relevant step, as technical reliability is a prerequisite for any implementation of care.
Survey instruments
Qualitative interviews were conducted before and after the intervention and analysed using Mayring’s structured content analysis. Quantitatively, the system usability scale (SUS) was used for care recipients; for carers, a specially developed questionnaire about integration into routine and perceived usefulness was used. In addition, technical stability was assessed indirectly via documented service interventions.
Key findings: High acceptance – benefits dependent on integration
Usability and acceptance among care recipients
The SUS evaluation resulted in a mean value of 78.6 (SD 9.8; n=20), which typically corresponds to a good to very good usability level. Item analyses indicate low perceived complexity and a high level of satisfaction overall. At the same time, there is a weak negative correlation between age and SUS score, which is consistent with qualitative statements: very elderly people were more likely to express uncertainty when using digital devices. In the interviews, a number of care recipients reported an increased sense of safety after five weeks, particularly due to the regular recording of vital data. Systems requiring little interaction (e.g. scales, sleeping mat) were described as particularly suitable for everyday use. Criticism was mainly levelled at devices requiring independent handling (smartwatch operation, unassisted blood pressure measurement). The need for more intensive support and a longer test duration was mentioned repeatedly.
Caregiver perspective: documentation gain vs concern about additional workload
At the beginning of the study, caregivers showed a positive attitude towards digital assistance, but were concerned that technology would add time and complexity to already complex processes. After the intervention, the benefits of the systematic collection and documentation of health data were emphasised in particular. However, the expectation of a noticeable reduction in the daily workload was relativised: the perceived effect depended heavily on how well the systems could be integrated into existing processes. The quantitative values reflect this: high levels of openness and positive attitudes contrast with relatively low approval ratings regarding physical, psychological and time relief. In free text responses, the benefits are explicitly linked to “saving time” and “reduction of administrative burden”. These findings underpin the study’s principal recommendation for implementation: technology is only useful if it actually supports rather than adds to routine processes.
Technical reliability as a real-world factor
were documented, 10 of which involved an on-site visit. The intervention rate is described as low and decreased over time – an indication that the system could be operated in a fundamentally stable manner under real-world conditions and that accompanying support processes were effective.
The SUS evaluation resulted in a mean value of 78.6 (SD 9.8; n=20), which typically corresponds to a good to very good usability level. Item analyses indicate low perceived complexity and a high level of satisfaction overall. At the same time, there is a weak negative correlation between age and SUS score, which is consistent with qualitative statements: very elderly people were more likely to express uncertainty when using digital devices. In the interviews, a number of care recipients reported an increased sense of safety after five weeks, particularly due to the regular recording of vital data. Systems requiring little interaction (e.g. scales, sleeping mat) were described as particularly suitable for everyday use. Criticism was mainly levelled at devices requiring independent handling (smartwatch operation, unassisted blood pressure measurement). The need for more intensive support and a longer test duration was mentioned repeatedly.
Caregiver perspective: documentation gain vs concern about additional workload
At the beginning of the study, caregivers showed a positive attitude towards digital assistance, but were concerned that technology would add time and complexity to already complex processes. After the intervention, the benefits of the systematic collection and documentation of health data were emphasised in particular. However, the expectation of a noticeable reduction in the daily workload was relativised: the perceived effect depended heavily on how well the systems could be integrated into existing processes. The quantitative values reflect this: high levels of openness and positive attitudes contrast with relatively low approval ratings regarding physical, psychological and time relief. In free text responses, the benefits are explicitly linked to “saving time” and “reduction of administrative burden”. These findings underpin the study’s principal recommendation for implementation: technology is only useful if it actually supports rather than adds to routine processes.
Technical reliability as a real-world factor
were documented, 10 of which involved an on-site visit. The intervention rate is described as low and decreased over time – an indication that the system could be operated in a fundamentally stable manner under real-world conditions and that accompanying support processes were effective.
The crucial point in fall prevention: monitoring alone is not enough
The study addresses fall prevention as a multidimensional process. Fall risk is not only the result of individual vital parameters, but also a reflection of functional performance, everyday activity, balance, strength and responsiveness – factors that can only be influenced to a limited extent by measurement, but can potentially be influenced by targeted intervention. This is precisely where the role of movement-based assistance becomes visible.
Many digital systems in home care primarily supply data. Data can convey security, improve progress monitoring and enable early warning signals. However, the therapeutically relevant “leap” only occurs when data is translated into actions: adaptation of measures, motivation to get active and targeted training. Against this background, the integration of an exercise machine such as the THERA-Trainer is not just another component, but a conceptual addition: it closes the gap between risk detection and risk modification.
Many digital systems in home care primarily supply data. Data can convey security, improve progress monitoring and enable early warning signals. However, the therapeutically relevant “leap” only occurs when data is translated into actions: adaptation of measures, motivation to get active and targeted training. Against this background, the integration of an exercise machine such as the THERA-Trainer is not just another component, but a conceptual addition: it closes the gap between risk detection and risk modification.
The benefits of the THERA-Trainer in the CARE REGIO concept: interventional, open to integration, data-capable
Even if the study is not designed as an effectiveness test for a single device, a technically robust line of argumentation on the role of the THERA-Trainer can be derived from the structure, objectives and result patterns.
Movement as a primary logic of prevention
The group of authors explicitly situates the intervention in the prevention paradigm. Especially in the home setting, where external training programmes are often unavailable, low-threshold, guided forms of training are becoming increasingly important. The THERA-Trainer addresses precisely this care barrier: it enables structured training in the home and can therefore – in the logic of the study – contribute to the prevention of loss of function and the need for care.
Practicality and user-friendliness as central determinants of acceptance
The results show a clear preference for systems that can be integrated into everyday life without major operating requirements. Compared to complex wearables or measuring devices, a movement exerciser is often less cognitively demanding: training can be established as a routine, without menu guidance, app navigation or frequent interaction steps. This aspect is important in the very elderly collective, as usability problems lead to users dropping out particularly quickly.
Training becomes visible and manageable within care
The DIP not only enables the display of vital data, but also of training data. This creates additional benefits for care teams: activity is not only recommended, but it can be documented. This enables changes in training adherence, possible declines in activity or even positive developments to be recognised at an early stage and translated into discussions, adjustments or motivational interventions. In an outpatient system that is heavily characterised by time constraints, this transparency can help to set priorities and make preventative measures more focused.
Movement as a primary logic of prevention
The group of authors explicitly situates the intervention in the prevention paradigm. Especially in the home setting, where external training programmes are often unavailable, low-threshold, guided forms of training are becoming increasingly important. The THERA-Trainer addresses precisely this care barrier: it enables structured training in the home and can therefore – in the logic of the study – contribute to the prevention of loss of function and the need for care.
Practicality and user-friendliness as central determinants of acceptance
The results show a clear preference for systems that can be integrated into everyday life without major operating requirements. Compared to complex wearables or measuring devices, a movement exerciser is often less cognitively demanding: training can be established as a routine, without menu guidance, app navigation or frequent interaction steps. This aspect is important in the very elderly collective, as usability problems lead to users dropping out particularly quickly.
Training becomes visible and manageable within care
The DIP not only enables the display of vital data, but also of training data. This creates additional benefits for care teams: activity is not only recommended, but it can be documented. This enables changes in training adherence, possible declines in activity or even positive developments to be recognised at an early stage and translated into discussions, adjustments or motivational interventions. In an outpatient system that is heavily characterised by time constraints, this transparency can help to set priorities and make preventative measures more focused.
Feedback on the THERA-Trainer tigo
Many participants rated the movement exerciser positively overall, as shown by the qualitative analysis of the interviews. They found it easy to use and described the device as useful. Some of them even considered acquiring their own trainer. This is reflected in statements from the interviews such as: “Positive – the trainer. I’ll see about getting one. It really has a good story to tell. Prophylaxis. It just made me feel a bit stronger.”
Many participants rated the movement exerciser positively overall, as shown by the qualitative analysis of the interviews. They found it easy to use and described the device as useful. Some of them even considered acquiring their own trainer. This is reflected in statements from the interviews such as: “Positive – the trainer. I’ll see about getting one. It really has a good story to tell. Prophylaxis. It just made me feel a bit stronger.”
Multiplier effect via relatives and professional support
The study describes how acceptance and longterm use depend heavily on social and professional support. For a training system, this means that the THERA-Trainer unleashes its potential in particular when guidance, motivation and, if necessary, support (from caregivers, therapists or relatives) are guaranteed.
The study describes how acceptance and longterm use depend heavily on social and professional support. For a training system, this means that the THERA-Trainer unleashes its potential in particular when guidance, motivation and, if necessary, support (from caregivers, therapists or relatives) are guaranteed.
The evaluation of the training in particular seemed to have a motivating effect. “Yes, the cycling is great. And I can see how far I’ve travelled.” Of course, regular movement training is particularly useful, which is why it is an advantage if this can be carried out at home at any time: “But I usually do the five kilometres or 15 minutes twice a day. That feels really good.”
Discussion: Implementation conditions as the actual effect factor
The study delivers a typical but important result in healthcare research: the perceived benefits of digital systems depend less on their technological performance than on the quality of their implementation. These include:
•Needs-based selection of systems together with those affected
• Training and continuous support
• Integration into routines and documentation processes
• Reliable interoperability and low maintenance requirements
These factors are not “add-ons”, but core elements of the intervention. From the perspective of a movement-orientated system such as the THERA-Trainer, this leads to a clear conclusion. What matters is not just that training is possible, but that it is guided, motivating, safe and embedded in the service delivery process. In a connected setting, the THERA-Trainer can be seen not only as a training device, but also as a component of an integrated prevention programme.
Limitations and categorisation
The group of authors rightly points out the limited generalisability: small sample, non-representative setting, limited subgroup analyses. Furthermore, the study was not designed to evaluate clinical endpoints such as fall frequency, mobility measures or functional scores. The evidence therefore primarily relates to implementation and acceptance: it shows that networked systems can be used under everyday conditions and which conditions determine their acceptance and perceived usefulness. However, this is particularly important for the introduction in healthcare contexts, because a lack of acceptance and process interruptions are often the main reasons why digital innovations fail.
•Needs-based selection of systems together with those affected
• Training and continuous support
• Integration into routines and documentation processes
• Reliable interoperability and low maintenance requirements
These factors are not “add-ons”, but core elements of the intervention. From the perspective of a movement-orientated system such as the THERA-Trainer, this leads to a clear conclusion. What matters is not just that training is possible, but that it is guided, motivating, safe and embedded in the service delivery process. In a connected setting, the THERA-Trainer can be seen not only as a training device, but also as a component of an integrated prevention programme.
Limitations and categorisation
The group of authors rightly points out the limited generalisability: small sample, non-representative setting, limited subgroup analyses. Furthermore, the study was not designed to evaluate clinical endpoints such as fall frequency, mobility measures or functional scores. The evidence therefore primarily relates to implementation and acceptance: it shows that networked systems can be used under everyday conditions and which conditions determine their acceptance and perceived usefulness. However, this is particularly important for the introduction in healthcare contexts, because a lack of acceptance and process interruptions are often the main reasons why digital innovations fail.
Conclusion: Networking is the means – movement is the goal
CARE REGIO provides compelling evidence that digital assistance systems in outpatient care do not fail due to the fundamental willingness of thoseinvolved, but due to practical issues: usability, support, process integration. At the same time, it is clear that fall prevention requires more than just vital data monitoring. Preventive added value arises where systems not only observe, but also enable action. Within this framework, the THERA-Trainer fulfils a specific, clinically justifiable role: it represents the transition from data to intervention, and thereby encapsulates the fundamental objectives of fall prevention in daily practice – preserving mobility, facilitating activity and decelerating functional deterioration. In a connected setting, training also becomes visible and can therefore be integrated into decision making processes relating to nursing and therapy. Under the implementation conditions identified in the study, the THERA-Trainer can therefore be considered a central component of a prevention system with real-world integration capability.
Feedback on the THERA-Trainer tigo
The qualitative evaluation also shows that several subjects reported that using the trainer had a positive impact on their well-being. Better mobility, a feeling of safety, increased activity and better sleep were mentioned. This was illustrated by statements such as: “I felt much more confident, especially with walking. I walked more (...) and then I cycled and then I felt much better and also slept much better.”
The qualitative evaluation also shows that several subjects reported that using the trainer had a positive impact on their well-being. Better mobility, a feeling of safety, increased activity and better sleep were mentioned. This was illustrated by statements such as: “I felt much more confident, especially with walking. I walked more (...) and then I cycled and then I felt much better and also slept much better.”
Jakob Tiebel
Health Business Consultant
Jakob Tiebel is OT and studied applied psychology with a focus on health economics. He has clinical expertise from his previous therapeutic work in neurorehabilitation. He conducts research and publishes on the theory-practice transfer in neurorehabilitation and is the owner of an agency for digital health marketing.
References:
- Gaßner, M., Hechtl, A., Nigg, U., Schmid, S., Yagci, S., & Friedrich, P. (2025). Digital assistants for outpatient care: benefits of intelligent connected assistive systems for caregivers and elderly people. Procedia Computer Science, 270, 4686–4695. https://doi.org/10.1016/j.procs.2025.09.594
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.