
THERAPY-Magazin
PAD – arm training for the legs?
Discover how arm ergometer training boosts walking distance and quality of life in PAD patients—even in advanced stages. A proven, pain-free alternative to treadmill therapy.

Raphael Weidmann
Physiotherapist
Peripheral artery disease (PAD) is an increasingly common disease in today's society. The current gold standard in physiotherapeutic PAD treatment is gait training on a treadmill or bicycle ergometer training [1, 6]. However, new findings show that training on an arm ergometer can have at least the same positive effects on walking distance and quality of life without triggering ischaemia-related claudication pain in the legs [8 – 11].
Theory
Peripheral artery disease is preceded by arteriosclerotic changes in more than 95% of cases. Even the smallest damage to the inner wall of the artery leads to chronic inflammatory processes, resulting in deposits of arteriosclerotic plaques. This reduces the arterial diameter and thus causes reduced blood circulation in the extremities. Classic risk factors are smoking, high blood pressure, diabetes mellitus, fat metabolism disorders and being overweight [3, 5].
The disease manifests in the lower extremities in over 90% of cases. Asymptomatic PAD has a prevalence of 15 %, and symptomatic PAD of 5 %, among the German population [3].
Peripheral artery disease is preceded by arteriosclerotic changes in more than 95% of cases. Even the smallest damage to the inner wall of the artery leads to chronic inflammatory processes, resulting in deposits of arteriosclerotic plaques. This reduces the arterial diameter and thus causes reduced blood circulation in the extremities. Classic risk factors are smoking, high blood pressure, diabetes mellitus, fat metabolism disorders and being overweight [3, 5].
The disease manifests in the lower extremities in over 90% of cases. Asymptomatic PAD has a prevalence of 15 %, and symptomatic PAD of 5 %, among the German population [3].
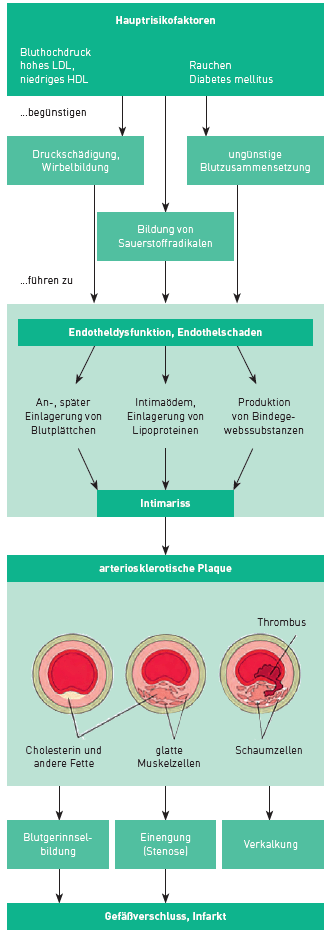
Abbildung 1: Risikofaktoren, Pathogenese und Folgen der Arteriosklerose [5]
At a glance Summarised
1.Peripheral artery disease (PAD) is becoming increasingly common. It affects the lower extremities in over 90 % of cases and is usually treated with bicycle ergometer or treadmill training.
2.In the disease, plaque is deposited on the inner wall of the artery, causing blood circulation to deteriorate. The disease is facilitated by smoking, high blood pressure and obesity, among other factors.
3.Several studies have investigated the effects of arm ergometer training on the maximum and pain-free walking distance of patients. Compared to treadmill or bicycle ergometer training, patients with arm ergometer training achieve similar or better results with regard to walking distance and subjectively perceived quality of life.
1.Peripheral artery disease (PAD) is becoming increasingly common. It affects the lower extremities in over 90 % of cases and is usually treated with bicycle ergometer or treadmill training.
2.In the disease, plaque is deposited on the inner wall of the artery, causing blood circulation to deteriorate. The disease is facilitated by smoking, high blood pressure and obesity, among other factors.
3.Several studies have investigated the effects of arm ergometer training on the maximum and pain-free walking distance of patients. Compared to treadmill or bicycle ergometer training, patients with arm ergometer training achieve similar or better results with regard to walking distance and subjectively perceived quality of life.
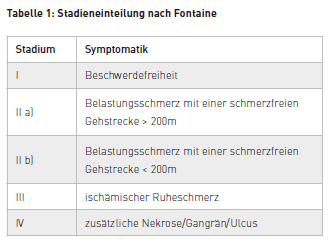
The condition is most often categorised according to Fontaine's staging scheme [3]:
Methodology
A literature search carried out on various health-specific databases yielded four relevant studies [8 – 11]. All four studies examined the effects of arm ergometer training on maximum and pain-free walking distance. In addition, one study investigated the effects on subjective quality of life, and another investigated the effects on oxygen saturation in the calf muscles. In order to assess the quality of the four studies, the PEDro score and an assessment grid for quantitative studies by Law et al. (1998) were used [2, 7].
Two studies can be rated as high quality and two as mediocre.
A literature search carried out on various health-specific databases yielded four relevant studies [8 – 11]. All four studies examined the effects of arm ergometer training on maximum and pain-free walking distance. In addition, one study investigated the effects on subjective quality of life, and another investigated the effects on oxygen saturation in the calf muscles. In order to assess the quality of the four studies, the PEDro score and an assessment grid for quantitative studies by Law et al. (1998) were used [2, 7].
Two studies can be rated as high quality and two as mediocre.
Discoveries
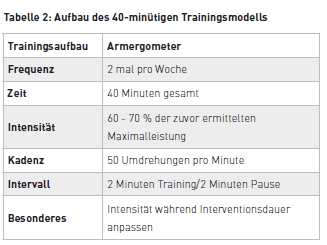
In the different intervention groups, arm ergometer training was compared with treadmill training, bicycle ergometer training and the combination of arm ergometer and treadmill training. In addition, a control group was present in each study. All intervention groups trained in a form of interval endurance training in which the intensity was adapted to the maximum personal performance of the subjects. Training took place either twice a week for 40 minutes or three times a week for 60 minutes under supervision.
After the interventions, significant improvements in walking distance were observed in the arm ergometer groups. In comparison with the treadmill or bicycle ergometer groups, similar or even better results were revealed. Based on the initial value, the pain-free walking distance in the arm ergometer groups could be increased by 33 to 83 % and the maximum walking distance by 29 to 53 %.
An astounding change in quality of life could also be observed. Patients who trained on the arm ergometer showed a significant improvement in their subjective quality of life after only six weeks. By contrast, fewer improvements were measurable in the bicycle ergometer group, and these could only be recorded 24 weeks after the start of training. The arm ergometer group was also better able to maintain this increased quality of life in the follow-up measurement after 72 weeks.
The researchers of one study wanted to use the oxygen measurement in the calf musculature to draw conclusions about blood circulation. The time to minimal oxygen saturation in the blood was measured by infrared sensors on the skin. After 12 weeks of training on the arm ergometer, the time to minimum oxygen saturation had been demonstrably increased by 65 %. This improvement could be due to increased blood flow to the lower extremity, but also to improved endothelial function or an increased ratio of capillaries to muscle fibres. Based on these facts, the question cannot be answered definitively – only further hypotheses regarding the effect on peripheral blood circulation can be made.
In the different intervention groups, arm ergometer training was compared with treadmill training, bicycle ergometer training and the combination of arm ergometer and treadmill training. In addition, a control group was present in each study. All intervention groups trained in a form of interval endurance training in which the intensity was adapted to the maximum personal performance of the subjects. Training took place either twice a week for 40 minutes or three times a week for 60 minutes under supervision.
After the interventions, significant improvements in walking distance were observed in the arm ergometer groups. In comparison with the treadmill or bicycle ergometer groups, similar or even better results were revealed. Based on the initial value, the pain-free walking distance in the arm ergometer groups could be increased by 33 to 83 % and the maximum walking distance by 29 to 53 %.
An astounding change in quality of life could also be observed. Patients who trained on the arm ergometer showed a significant improvement in their subjective quality of life after only six weeks. By contrast, fewer improvements were measurable in the bicycle ergometer group, and these could only be recorded 24 weeks after the start of training. The arm ergometer group was also better able to maintain this increased quality of life in the follow-up measurement after 72 weeks.
The researchers of one study wanted to use the oxygen measurement in the calf musculature to draw conclusions about blood circulation. The time to minimal oxygen saturation in the blood was measured by infrared sensors on the skin. After 12 weeks of training on the arm ergometer, the time to minimum oxygen saturation had been demonstrably increased by 65 %. This improvement could be due to increased blood flow to the lower extremity, but also to improved endothelial function or an increased ratio of capillaries to muscle fibres. Based on these facts, the question cannot be answered definitively – only further hypotheses regarding the effect on peripheral blood circulation can be made.
Practice transfer
In conclusion, a positive recommendation can be given for arm ergometer training for patients with stage II PAD according to Fontaine for improving pain-free and maximum walking distance, as well as for improving subjective quality of life. The 40-minute training model is recommended for implementation in everyday practice. It has a similar effect to the 60-minute model, but is less time-consuming to perform.
Arm ergometer training could also have great potential for patients with stage III PAD according to Fontaine. Due to the ischaemic rest pain, training of the legs is contraindicated and the patients are often bed-bound. Patients confined to bed only rarely have the opportunity to undergo training to prevent thrombosis and increase cardiopulmonary endurance, even though suitably adapted endurance training has been proven to have positive effects on the cardiovascular system and the associated mortality risk. Here, many patients could benefit from suitable arm ergometer training devices and actively improve their prognosis.
Arm ergometer training is thus an effective alternative and could increase the compliance of those affected [8 – 11].
In conclusion, a positive recommendation can be given for arm ergometer training for patients with stage II PAD according to Fontaine for improving pain-free and maximum walking distance, as well as for improving subjective quality of life. The 40-minute training model is recommended for implementation in everyday practice. It has a similar effect to the 60-minute model, but is less time-consuming to perform.
Arm ergometer training could also have great potential for patients with stage III PAD according to Fontaine. Due to the ischaemic rest pain, training of the legs is contraindicated and the patients are often bed-bound. Patients confined to bed only rarely have the opportunity to undergo training to prevent thrombosis and increase cardiopulmonary endurance, even though suitably adapted endurance training has been proven to have positive effects on the cardiovascular system and the associated mortality risk. Here, many patients could benefit from suitable arm ergometer training devices and actively improve their prognosis.
Arm ergometer training is thus an effective alternative and could increase the compliance of those affected [8 – 11].
Cycling
Fachkreise
mobi
Science
THERAPY 2019-II
THERAPY Magazine
tigo
Raphael Weidmann
Physiotherapist
Raphael Weidmann is a physiotherapist who, together with his fellow student Erik Willems, conducted research on the effects of cyclical movement training on patients with PAD (Peripheral Artery Disease).
Erik Willems
Physiotherapist
Erik Willems is a physiotherapist who, together with his fellow student Raphael Weidmann, conducted research on the effects of cyclical movement training on patients with PAD (Peripheral Artery Disease).
References:
- Beise U. (2011). Guidelines – Periphere arterielle Verschlusskrankheit (PAVK). Heruntergeladen von www.medix.ch/wissen/ guidelines/herz-kreislauf-erkrankungen/pavk.html am 12.09.2017.
- Hegenscheidt S., Harth A., Scherfer E. (2010). PEDro-Skala- Deutsch. Heruntergeladen von www.pedro.org.au/wp-content/uploads/PEDro_scale_german.pdf am 07.08.2017.
- Herold G. (2018). Innere Medizin. Köln: Gerd Herold Verlag.
- Hofmann P., Tschakert G., Wonisch M., Pokan R. (2009). Journal für Kardiologie – Austrian Journal of Cardiology; 16 (9-10), 333-336.
- Huch R., Jürgens K. D. (2015). Mensch Körper Krankheit. München: Elsevier GmbH Urban & Fischer.
- Jäger K. A., Amann-Vesti B., Banyai M., Baumgartner I., Bounameaux H., Frauchiger B., Desalmand D. (2007). Schweizer Richtlinien zum Management von PAVK-Patienten durch den Facharzt. Heruntergeladen von www.angioweb.ch/de/Guidelines am 21.07.2017.
- Law M., Stewart D., Pollock N., Letts L., Bosch J., Westmorland M. (1998). Formular zur kritischen Besprechung quantitativer Studien. Heruntergeladen von srs-mcmaster.ca/wp-content/ uploads/2015/04/Critical-Review-Form-Quantitative-Studies- German.pdf am 07.08.2017.
- Saxton J. M., Zwierska I., Blagojevic M., Choksy S., Nawaz A., Pockley G. (2011). Upper- versus lower-limb aerobic exercise training on health-related quality of life in patients with symptomatic peripheral arterial disease. Vascular Surgery(53), S. 1265-1273.
- Tew G., Nawaz S., Zwierska I., Saxton J. M. (2009). Limb-specific and cross-transfer effects of arm-crank exercise training in patients with symptomatic peripheral arterial disease. Clinical Science(117), S. 405-413.
- Treat-Jacobson D., Bronas U. G., Leon A. S. (2009). Efficacy of arm-ergometry versus treadmill exercise training to improve walking distance in patients with caludication. Journal of Vascular Medicine(14), S. 203-213.
- Zwierska I., Walker R. D., Choksy S. A., Male J. S., Pockley A. G., Saxton J. M. (2005). Upper- vs. lower-limb aerobic exercise rehabilitation in patients with symptomatic peripheral arterial disease: A randomized control trial. Journal of Vascular Surgery (42), S. 1122-1130.
Related contents
Find related exciting contents in our media library.
Mehr laden
This is not what you are searching for? Knowledge
Meet our specialists.
Are you interested in our solutions? Schedule a meeting with a Consultant to talk through your strategy and understand how TEHRA-Trainer can help you to advance rehabilitation.
You need to load content from reCAPTCHA to submit the form. Please note that doing so will share data with third-party providers.
More InformationYou are currently viewing a placeholder content from Turnstile. To access the actual content, click the button below. Please note that doing so will share data with third-party providers.
More Information